
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Neutropaenic enterocolitis with severe aplastic anaemia
Sheehan T1 ; Hassan Akhtar1 *; Bhutta S1 ; Saleem S2 ; D O’Keeffe2 ; Kiely P3 ; Skelly MM1
1Department of Gastroenterology, University Hospital Limerick, Ireland.
2Department of Haematology, University Hospital Limerick, Ireland
3Department of Radiology, University Hospital Limerick, Ireland.
*Corresponding Author : Hassan Akhtar
Department of Gastroenterology, University
Hospital Limerick, Ireland.
Email: dr.hassanakhtar121@gmail.com
Received : Jan 03, 2025
Accepted : Jan 24, 2025
Published : Jan 31, 2025
Archived : www.jcimcr.org
Copyright : © Akhtar H (2025).
Abstract
Presentation: 55-year-old female presented complaining of symptoms of loose bowel motions, crampy abdominal pain, and fever for 3 days. She has a background medical history of Crohn’s disease, Rheumatoid Arthritis, and previous PCP pneumonia. Medications of note included Methotrexate and Sulfamethoxazole-Trimethoprim for PCP prophylaxis.
Diagnosis: Bloods results revealed a pancytopaenia. CT abdomen reported as severe pancolitis. Bone marrow aspiration showed aplastic anaemia under microscopy.
Treatment: Managed in ITU, with mechanical ventilation and vasopressors. She was on multiple antibiotics and antifungals guided by Microbiology. Romiplostim advised by Haematology was key to patient recovery.
Discussion/conclusion: The combination of Methotrexate and Sulfamethoxazole-Trimethoprim has a well-established risk of causing bone marrow suppression. The use of Romiplostim was a point of interest in this case.
Citation: Sheehan T, Akhtar H, Bhutta S, Saleem S, O’Keeffe D, et al. Neutropaenic enterocolitis with severe aplastic anaemia. J Clin Images Med Case Rep. 2025; 6(1): 3448.
Introduction
Neutropaenic enterocolitis or Typhlitis is a life threating emergency, usually encountered post chemotherapy or patients with blood related cancers. Pathogenesis involves deposition of lymphoproliferative cells that infiltrate mucosa [1] and cause ulcerations. Superimposed bacterial or fungal infections contribute to mucosal injury. The incidence is disputed, with ranges as wide as 0.8-26% [2] reported. However, Methotrexate as well as other cytotoxic medications are a recognised risk factor. CT is the imaging modality of choice in these cases [2]. Historically, early surgical management of typhlitis was deemed to give best chance of survival, which used to be to be viewed as a terminal disease. Now surgical management is reserved, and medical management is now preferred in these cases due to improvement in supportive care.
Case report
A 55-year-old female presented to the Emergency department complaining of extreme fatigue, crampy abdominal pain, watery diarrhoea, vomiting and intermittent fever for 3 days. Her previous medical history includes Crohn’s disease for which she is prescribed weekly methotrexate 20 mg, folate supplementation, and prednisolone 10 mg maintenance dose. She had a previous ICU admission with PCP pneumonia and acute autoimmune hepatitis. Because of this, she remained on prophylactic Sulfamethoxazole-Trimethoprim. On arrival to ED the patient met SIRS criteria. The sepsis protocol was initiated, and the patient was placed on high-flow oxygen, intravenous crystalloids administered, and a urinary catheter was placed. Initial investigations revealed a raised CRP (256). FBC showed evidence of pancytopaenia. She was particularly neutropaenic (0.05x109 /L) and thrombocytopaenic (40x109 /L). The patient was in type 2 respiratory failure on arterial blood gas on admission. A CT Abdomen/Pelvis reported findings consistent with severe pancolitis and proctitis and enteritis.

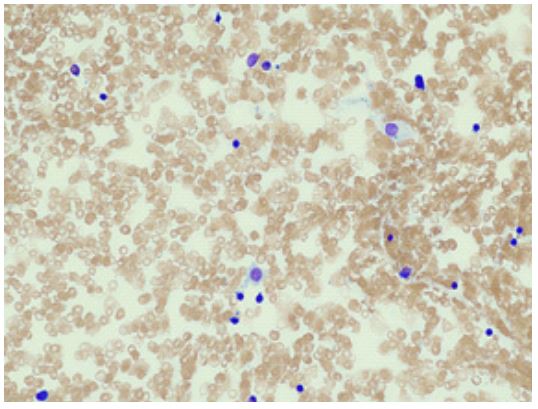
Microbiology was consulted and she was prescribed IV meropenem and PO Vancomycin. A bone marrow biopsy was performed.
The result of BMA is suspected to be due to bone marrow suppression from co-prescription of methotrexate and Sulfamethoxazole-Trimethoprim. Rescue therapy with IV folinic acid was given. Increased levels of folinic acid potentiate the cytotoxic effects of-FU in the cell [3]. Further deterioration led to mechanical ventilation. There was also an escalation of antibiotic therapy to include Metronidazole, Tigecycline, Daptomycin and Caspofungin for fungal cover. A decision was made to give Romiplostim, a platelet growth factor, that has been associated with rapid bone marrow recovery. The next 2 days showed a remarkable improvement of neutrophil and platelet count. She was no longer pancytopenia. She remained on multiple IV antibiotics. This improvement led to extubation 5 days later. She was eventually stepped down to ward level care for rehabilitation. She was maintained on PO Eltrombopag, a thrombopoetin receptor antagonist.
Discussion
The combination of Methotrexate and Sulfamethoxazole-Trimethoprim has a well-established risk of causing bone marrow suppression. There are many published cases outlining the severe interactions of these drugs, mainly resulting in life threatening myelosuppression, mucositis and nephrotoxicity [4]. This is the most likely cause of the patients severe aplastic anaemia. The unlicensed use of Romiplostim in the treatment of severe aplastic anaemia is the key point of interest in this case. In severe aplastic anaemia, for which Eltrombopag has been licenced in combination with immunosuppressive therapy, a similar study showed similar efficacy of Romiplostim [5]. In addition to this, a case reported in this year gave anecdotal evidence that the immunomodulatory effect of Eltrombopag could decrease the inflammatory response of IBD [6].
Conflicts of interests: The authors have no conflicts of interests to declare.
References
- Neutropenic enterocolitis: A continuing medical and surgical challenge. NO Machado, MS, FRCSEd. 2010.
- L Nesher, Kenneth VI. Neutropenic enterocolitis, A growing concern in the era of widespread use of aggressive chemotherapy. 2013.
- Folinic Acid, Yana D. Gristan, L Moosavi. 2021.
- Methotrexate and trimethoprim-sulfamethoxazole, Toxicity from this combination continues to occur. J Cudmore.2014
- Bussel JB, Soff G, Balduzzi A. A review of romiplostim mechanism of action and clinical applicability. 2021.
- Elabbass Abdelmahmuod, Elrazi Awadelkarim, Hamid Ali. Eltrombopag and its beneficial role in the management of ulcerative Colitis associated with ITP as an upfront therapy case report. 2021.