
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
A benign mimic in the world of melanocytic lesions
Ji Fung Yong1 *; Stephen Crowther2 ; Anne-Marie Tobin1,3
1Department of Dermatology, Tallaght University Hospital, Dublin, Ireland.
2Department of Histopathology, Tallaght University Hospital, Dublin, Ireland.
3Trinity College Dublin, Dublin, Ireland.
*Corresponding Author : Ji Fung Yong
Department of Dermatology, Tallaght University
Hospital, Dublin, Ireland.
Email: jifungyong@gmail.com
ORCID: https://orcid.org/0009-0000-5243-7413
Received : Jan 03, 2025
Accepted : Jan 24, 2025
Published : Jan 31, 2025
Archived : www.jcimcr.org
Copyright : © Yong JF (2025).
Abstract
Spitz naevus, although benign, can often mimic melanoma due to their rapid growth, changing appearance, and variable pigmentation. Recognising the distinct characteristics may aid to differentiate spitz naevi from other melanocytic lesions. Despite the benign nature of Spitz naevus, any changing pigmented lesion warrants excision and histopathologic examination due to the risk of melanoma. A tailored approach considering patient risk factors (such as Fitzpatrick skin type, history of sun exposure, and blistering sunburns) and lesion characteristics is important for appropriate management.
Keywords: Melanocytic lesion; Spitz naevus; Dermatology; Pathology.
Citation: Yong JF, Crowther S, Tobin AM. A benign mimic in the world of melanocytic lesions. J Clin Images Med Case Rep. 2025; 6(1): 3449.
Description
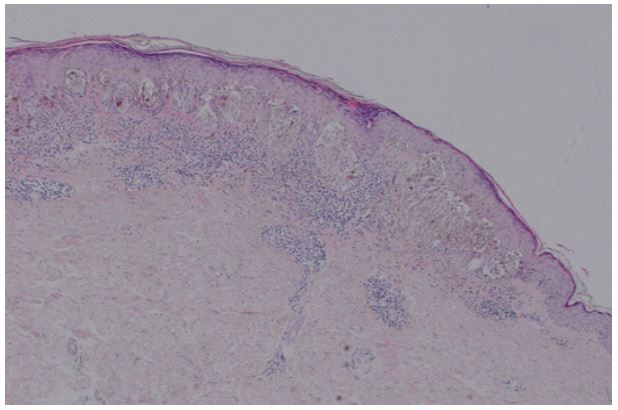
A 43-year-old White woman presented with a 2-month history of enlarging mole which was first noted six months ago on her left upper arm. She had Fitzpatrick type II skin, had taken approximately 15 sun holidays and had previous blistering sunburn. Examination showed a 6x4 mm symmetrical, regular pigmented lesion on the left upper arm. Dermoscopy revealed homogenous brown pigmentation with grey-white lines in the centre of the lesion and peripheral pseudopods. An excisional biopsy of this lesion confirmed the diagnosis of Spitz Naevus (SN). SN is a benign melanocytic neoplasm of epitheloid and/ or spindle melanocytes, which typically presents in childhood but may occur at any age. They tend to grow rapidly within the first six months, reaching a size of approximately 1 cm, and remaining static thereafter [1]. Common clinical features include a small diameter (less than 5-6 mm), dome-shaped papule, small plaque, or macule, with colours ranging from pink and red to various shades of brown. Dermoscopy demonstrates a starburst pattern consisting of a hyperpigmented centre with symmetrically distributed peripheral pseudopods and/or streaks, or a globular pattern with reticular depigmentation [2]. Histopathologically, SN can be categorized as junctional, compound or dermal, similar to other types of melanocytic naevi. SN is usually composed predominantly of spindled or epitheli oid cells with abundant cytoplasm, with few mitoses, occurring in the mid-upper part of the lesion. Melanin may be absent or symmetrically distributed, and is typically absent in the deepest part of the lesion. A lymphocytic infiltrate may be present at the perivascular and at the base, but it does not mix with the melanocytes [3]. Immunohistochemistry demonstrates retained p16 expression, negative PRAME (Preferentially Expressed Antigen in Melanoma) and no increase in Ki-67 expression in the dermal component. Management of SN is largely based on the dual goals of minimizing the risk of missing melanoma and avoiding unnecessary excisions of benign moles [2]. Regular monitoring of static SN is often appropriate in low-risk cases (non-nodular, symmetrical lesion with a starburst pattern and in patients less than 12-year-old [2]), however any changing pigmented lesion warrants excision for histopathologic examination to avoid missing a melanoma diagnosis.


Declarations
Conflict of interests: The authors declared no potential conflicts of interest.
Informed consent: The patient in this manuscript has given written informed consent to the publication of the case details and clinical images.
References
- Brown A, Sawyer JD, Neumeister MW. Spitz Nevus: Review and Update. Clin Plast Surg. 2021; 48(4): 677-686. doi: 10.1016/j. cps.2021.06.002.
- Lallas A, Apalla Z, Ioannides D, et al. Update on dermoscopy of Spitz/Reed naevi and management guidelines by the International Dermoscopy Society. Br J Dermatol. 2017; 177(3): 645- 655. doi:10.1111/bjd.15339.
- Stefanaki C, Stefanaki K, Chardalias L, Soura E, Stratigos A. Differential diagnosis of Spitzoid melanocytic neoplasms. J Eur Acad Dermatol Venereol. 2016; 30(8): 1269-1277. doi:10.1111/ jdv.13665.