
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Acute lower limb ischemia in neonates: A case report
Soraya Hani*; Najwa IMAD; Soufiane El Moussaoui; Widad Lahmini; Mounir Bourrouss
Paediatric Emergency Department, Mother and Child Hospital, Mohammed VI University Hospital, Marrakech, Morocco.
*Corresponding Author : Soraya Hani
Paediatric Emergency Department, Mother and
Child Hospital, Mohammed VI University Hospital,
Marrakech, Morocco.
Email: dr.sorayahani@gmail.com
Received : Dec 13, 2024
Accepted : Jan 27, 2025
Published : Feb 03, 2025
Archived : www.jcimcr.org
Copyright : © Hani S (2025).
Abstract
Aortic thrombosis in newborns is rare and severe. It is often attributed to umbilical artery catheterization; however, its cause may be unknown in almost half of cases. The severity of the condition requires rapid and effective treatment. Although there are many therapeutic, there is no universally accepted course of action. We report the observation of an extensive thrombosis of the abdominal aorta in a newborn fifteen days old, revealed by ischaemia of the right lower limb. The thrombosis was not related to an umbilical catheterization. The diagnosis was confirmed by Doppler ultrasound and angioscan, the outcome was unfavourable, with death of the neonate in severe sepsis. With regard to this observation, a review of the literature concerning the epidemiological, clinical, therapeutic and evolutionary data of aortic thrombosis in the neonate is presented.
Keywords: Ischemia; Aortic thrombosis; Limb; Neonate.
Citation: Hani S, IMAD N, El Moussaoui S, Lahmini W, Bourrouss M. Acute lower limb ischemia in neonates: A case report. J Clin Images Med Case Rep. 2025; 6(2): 3451.
Introduction
Neonatal limb ischemia indeed poses significant challenges due to its rarity and varied presentation. Prompt diagnosis and management are crucial, given the spectrum of potential outcomes from asymptomatic incidents to life-threatening situations. However, despite the evolving nature of management strategies, there’s still a lack of solid evidence-based treatment algorithms in this area. This underscores the need for continued research and collaboration among medical professionals to improve outcomes for affected neonates [1,2].
Clinical observation
We present à case of a fifteen-day old male neonate, weigning 3800 grams, born to a 27 years old mother via vaginal delivry, with no particular medical history such as a miscarriage event or maternal diabetes. The patient was admitted to paediatric emergency with haemorrhagic syndrome and respiratory distress. Examination revealed palpebral ecchymosis and bilateral conjunctival haemorrhage, opisthotonos position, bulging anterior fontanel, Archaic reflexes and sucking reflexes were absent, tonic-type convulsions with myoclonus and chewing, the newborn also showed signs of respiratory struggle with bilateral crepitating rales and bradycardia. The second day after hospitalization, the newborn had swelling and ecchymotic right lower limb, (which began in the right feet and extended to the thighs over the next days. Right femoral pulse was diminished at first, becoming non palpable within the next hours, with a peripheral coldness and a prolonged capillary refill.
Preoperative biological assessment found a polycythemia with Hemoglobin (Hb) at 19.2 g/dL, Hematocrit (Hct) at 68.2% and a thombopenia at 21000/mm3, the sedimentation velocity was 2 at the 1st hour and 5 at the 2nd hour, C-Reactive Protein (CRP) came at 10 mg/l, Prothrombin Time (PT) count 60 % with an INR of 1.28, at last the fibrinogen came at 2,42 g/l.
Initial lower limbs doppler ultrasound revealed a peripheral arterial disease with an absence of the right lower limb blood flow
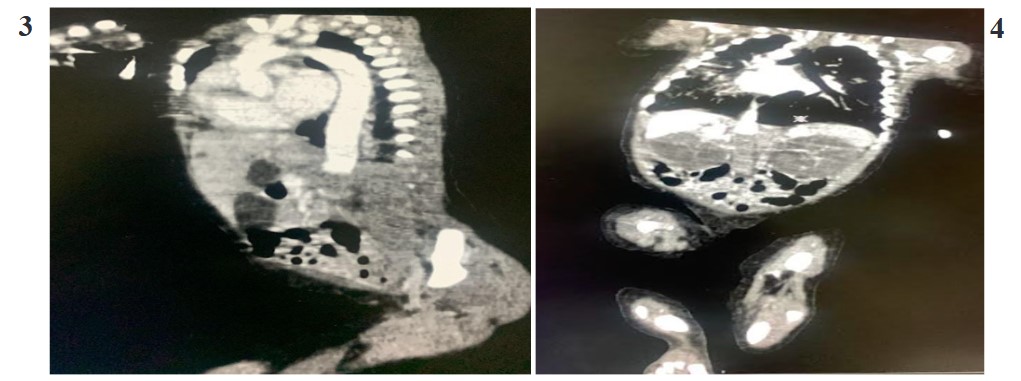
Echocardiography did not reveal any cardiac abnormalities. The diagnosis was completed with a thoracic-Abdominal and pelvic CT angiogram which revealed occlusion of the abdominal aorta, mesenteric arteries and renal arteries.
The patient was on Unfractionated Heparin (UFH) treatment starting at 100 U/kg, and because of thrombocytopenia one unit of platelets was transfused preoperatively. A bleeding of 40 ml was induced to minimize the risk of an additional thrombus because of the high hemoglobin level.
In order to identify the etiology of this condition, we have measured the C and S protein level, and the antithrombin III, however we couldn’t benefit from the results because of the early onset of heparin.
The neonate was died with severe hemorrhage.

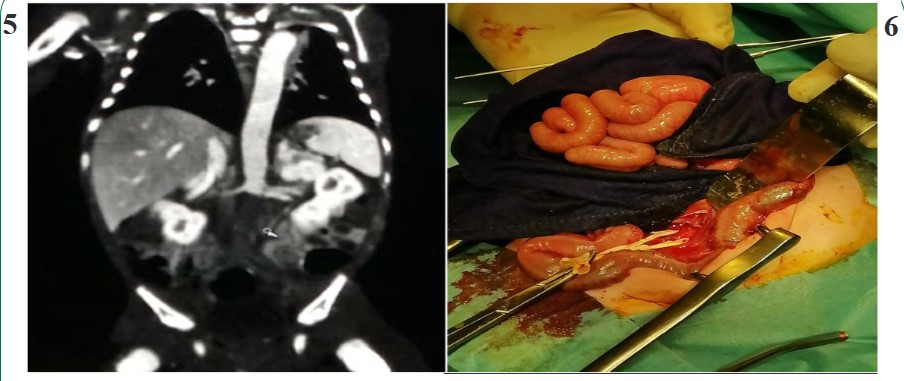
Figures 5: Peroperative individualization of the abdominal aorta.

Figures 7: Post operative appearance of the teft lower limbs

Figures 9: Post operative appearance of the left foot

Figures 11: Appearance of the left lower limb.

Figures 13: Appearance of the left foot after 15 days of treatment.
Discussion
Neonatal thromboembolism can indeed exhibit a wide range of manifestations, largely influenced by factors such as the location and size of the thrombus. While iatrogenic causes, particularly related to vascular catheterization, are common, spontaneous occurrences, such as aortic or renal vein thrombosis, are rare but documented [2,3]. Various risk factors contribute to the development of neonatal thromboembolism, including maternal conditions like diabetes and lupus, as well as neonatal factors such as polycythemia, dehydration, and coagulopathy [4-7]. In our case, polycythemia was the primary concern with-out any other apparent etiology.
Categorizing Thromboembolism (TE) in neonates into arterial, venous, and central nervous system events helps in understanding its varied presentations and implications. Arterial TE, which comprises approximately half of all cases in neonates [2], often presents with specific clinical features. Peripheral arterial occlusion, for instance, is characterized by the 6 Ps: pallor, pulselessness, paralysis, pain, paresthesia, and perishing cold of the affected extremity. However, the clinical presentation can vary depending on factors such as the site and timing of occlusion. Early recognition of these signs and symptoms is crucial for timely intervention and management to mitigate potentially life-threatening complications.
Events related to the arterial, venous, and central nervous systems will be classified as TE. Its manifestation can range from discrete or asymptomatic symptoms to potentially fatal consequences. The clinical characteristics of peripheral arterial occlusion are gathered as the 6P: pallor, pulselessness, paralysis, pain, parasthesia, and perishing cold of the involved extremity. Arterial vascular events account for approximately half of all TE in the neonatal population [2,8].
The most popular imaging method for diagnosing neonatal arterial or venous thrombosis is Doppler ultrasonography, which can show reduced flow in a partial occlusion and absence of flow in a complete one. Even in cases where the thrombus is not visible, abnormal arterial waveforms can serve as a diagnostic tool for partial or total arterial occlusion [9,10], using either echocardiography or abdominal ultrasound is also applied to confirm clinical suspicion of TE or to screen patients for clinically silent form [2].
Treatment guidelines for pediatric patients with TE events are typically extrapolated from the literature regarding adults, as neonatologists’ medical decisions regarding the management of neonatal TE emergencies were limited by the lack of randomized clinical trials [11]. The aim of treatment is to avoid life-threatening consequences, thrombus extension and recurrence, and long-term complications, all without significantly raising the risk of bleeding [12].
The American College of Chest Physicians Evidence Based Clinical Practice Guidelines presented a guideline strategy for the management of thrombosis in neonates and children, for neonates with acute femoral artery thrombosis, the guideline recommends Intravascular Unfractionated Heparin (UFH) the first line of treatment. In addition, long-term use of therapeutic UFH in children should be avoided. For neonates whose limb or organ are in danger and who do not respond to initial UFH therapy, thrombolysis is advised. When starting UFH therapy, UFH boluses should not exceed 75 to 100 units/kg, and they should be withheld or reduced if there are significant bleeding risks [13].
A review summarized the management of aortic thrombosis, therapeutic options include UFH or low molecular weight heparin (LMWH), thrombolytic therapy, and surgical thrombectomy, but there are insufficient data to recommend any one treatment over others, especially regarding spontaneous aortic thrombosis [14].
Conclusion
Spontaneous neonatal TE is a rare condition of uncertain cause that requires early diagnosis and management. Neonatologists and pediatricians should be aware of the first clinical signs in order to avoid limb and organ damage. Strategies for management are still evolving, we hope that more guidelines will be provided in order to improve the care given.
Conflict of interests: The authors declare no conflict of interests regarding those cases.
References
- A Arshad, MJ McCarthy. Management of Limb Ischaemia in the Neonate and Infant Eur J Vasc Endovasc Surg. 2009; 38: 61,65.
- Alex Veldman, Marcel F Nold, Ina Michel-Behnke. Thrombosis in the critically ill neonate: incidence, diagnosis, and management Vascular Health and Risk Management. 2008: 4(6): 1337-1348.
- Muhammad Aslam, Deborah Guglietti, Anne R Hansen. Neonatal Arterial Thrombosis at Birth: Case Report and Literature Review Am J Perinatol. 2008; 25: 347-352.
- Oppenheimer EH, Esterly JR. Thrombosis in the newborn: comparison between infants of diabetic and nondiabetic mothers J Pediatr. 1965; 67: 549.
- NE Wiseman, JN Briggs, VS Bolton. Neonatal Arterial Occlusion with Ischemic Limb Gangrene Journal of Pediafric Surgery. 1977; 12: 5.
- Boffa MC, Lachassinne E. Infant perinatal thrombosis and antiphospholipid antibodies: a review. 2007; 16(8): 634-641.
- Hathaway WE, Mull MM, Pechet GS, et al. Disseminated intravascular coagulation in the newborn. 1969; 43: 233.
- Samer Abdelrazeq, Abdullatif Alkhateeb, Hani Saleh, Haitham Alhasan, et al. Intrauterine Upper Limb Ischemia: An Unusual Presentation of Fetal Thrombophilia-A Case Report and Review of the Literature Hindawi Publishing Corporation Case Reports in Pediatrics. 2013; 670258.
- Cremin BJ, Davey H, Oleszczuk-Raszke K. Neonatal renal venous thrombosis: sequential ultrasonic appearances Clin Radiol. 1991; 44(1): 52-5510.
- Wright NB, Blanch G, Walkinshaw S, Pilling DW. Antenatal and neonatal renal vein thrombosis: new ultrasonic features with high frequency transducers. Pediatr Radiol. 1996; 26(9): 686- 689.
- A Saxonhouse. Management of Neonatal Thrombosis Matthew Clin Perinatol. 2012; 39: 191-208 doi: 10.1016/j.clp.2011.12.018.
- Romantsik O, Bruschettini M, Zappettini S, Ramenghi LA, Calevo MG. Heparin for the treatment of thrombosis in neonates. Cochrane Database of Systematic Reviews. 2016; 11: 012185. DOI: 10.1002/14651858.CD012185.pub2.
- Paul Monagle, Anthony KC Chan, Neil A Goldenberg, Rebecca N Ichord, et al. Vesely Antithrombotic Therapy in Neonates and Children Chest. 2012; 141(2): 737-801. doi: 10.1378/ chest.11-2308.
- Nagel K, Tuckuviene R, Paes B, Chan AK. Neonatal aortic thrombosis: a comprehensive review Klin Padiatr. 2010; 222(3): 134 -139.