
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Recurrence and metastasis of an AB-type thymoma 16 years post-surgical resection: A case report
Yu Liu; Linlin Deng; Xiangrong Yu*
Department of Radiology, Zhuhai People’s Hospital (Zhuhai Hospital Affiliated with Jinan University), Zhuhai, Guangdong, China.
*Corresponding Author : Xiangrong Yu
Department of Radiology, Zhuhai People’s Hospital
(Zhuhai Hospital Affiliated with Jinan University),
Zhuhai, Guangdong, China.
Tel: +86 135-3658-6162;
Email: yxr00125040@126.com
Received : Dec 02, 2024
Accepted : Jan 28, 2025
Published : Feb 04, 2025
Archived : www.jcimcr.org
Copyright : © Xiangrong Yu (2025).
Keywords: Thymoma; AB type; Recurrence; Metastasis.
Citation: Liu Y, Deng L, Yu Xiangrong. Recurrence and metastasis of an AB-type thymoma 16 years post-surgical resection: A case report. J Clin Images Med Case Rep. 2025; 6(2): 3452.
Introduction
AB-type thymomas are generally considered non-invasive tumors, with most cases classified as Masaoka stage I or II. These tumors exhibit indolent progression, and instances of recurrence or distant metastasis are exceptionally rare. Here, we present a case of AB-type thymoma that recurred at the original thymectomy site 16 years post-surgery, accompanied by pleural and pulmonary metastases.
Case presentation
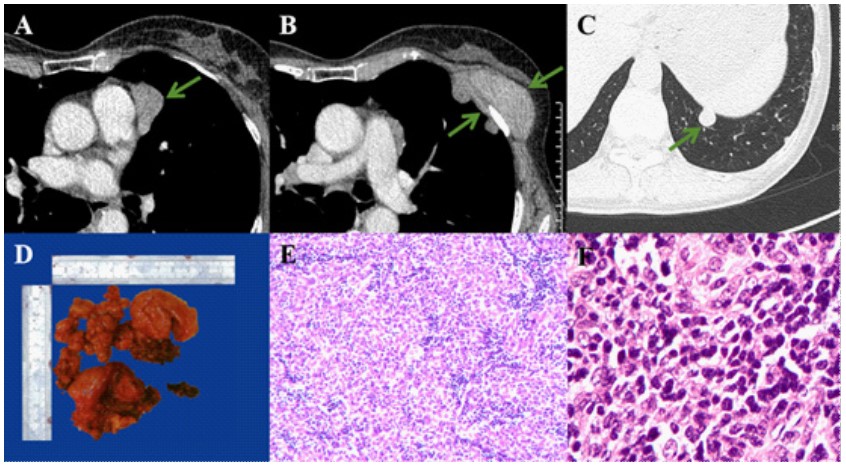
A 57-year-old female presented with a palpable mass on the left chest wall. Sixteen years earlier, at the age of 41, she had undergone surgical resection of a thymoma located in the anterior mediastinum. At that time, she was asymptomatic and showed no signs of myasthenia gravis. Upon her current admission, laboratory evaluations were unremarkable. Chest Computed Tomography (CT) revealed a large mass on the left anterior chest wall, irregular masses in the anterior mediastinum, and a round nodule in the lower lobe of the left lung (Figures 1A-1C). Surgical intervention included resection of the thymoma, excision of the chest wall mass, and removal of the pulmonary nodule. Gross examination of the resected specimens demonstrated multiple tumor masses (Figure 1D). Histopathological analysis with hematoxylin-eosin staining revealed spindle cells characteristic of type A thymoma and lymphocytes consistent with type B thymoma (Figures 1E). Certain type A regions exhibited atypical features such as nuclear enlargement, coarse chromatin, and occasional mitotic figures (Figures 1F). Pathological evaluation confirmed that the mediastinal, chest wall, and pulmonary lesions were all AB-type thymoma. The mediastinal lesion was diagnosed as recurrent thymoma, while the chest wall and pulmonary lesions were classified as pleural and lung metastases, respectively. Since the tumors were completely resected, no adjuvant therapy was administered.
Discussion/conclusion
Thymomas, originating from thymic epithelial cells, are the most prevalent tumors of the anterior mediastinum and account for 0.2% to 1.5% of all malignancies [1]. According to the WHO classification, thymomas are subdivided into types A, AB, B1, B2, and B3 [2]. AB-type thymomas are typically non-invasive and exhibit almost benign behavior, with the majority of cases classified as Masaoka stage I or II. For stage I thymomas, complete surgical resection is generally curative [3].
Postoperative recurrence or metastasis of AB-type thymomas is rare. Possible mechanisms include incomplete resection of thymic or ectopic thymic tissue and intraoperative tumor cell seeding [4]. Recurrence or metastasis generally manifests within months to a few years post-surgery. This case is notable for the recurrence at the thymectomy site and metastases to the pleura and lung 16 years postoperatively-a remarkably prolonged disease-free interval. Reported recurrence rates for non-invasive thymomas after complete resection range from 0% to 10%, commonly presenting as localized mediastinal recurrence or pleural dissemination [4]. Hematogenous spread is uncommon, with the lungs being the most frequent metastatic site, followed by bones and the liver [5].
In comparison with previously documented cases of metastatic thymoma, this patient had an unusually extended disease-free interval before recurrence and metastasis, ultimately experiencing a poor clinical outcome. Unfortunately, no standardized strategies currently exist to prevent distant metastasis. This case highlights the critical importance of vigilant long-term follow-up for thymoma patients to enable early detection and management of recurrence or metastasis.
References
- Engels E, Pfeiffer R. Malignant thymoma in the United States: Demographic patterns in incidence and associations with subsequent malignancies. International journal of cancer. 2003; 105(4): 546-51. doi: 10.1002/ijc.11099.
- Marx A, Chan J, Coindre J, Detterbeck F, Girard N, et al. The World Health Organization Classification of Tumors of the Thymus: Continuity and Changes. Journal of thoracic oncology: Official publication of the International Association for the Study of Lung Cancer. 2015; 10(10): 1383-95. doi: 10.1097/ jto.0000000000000654.
- Gamboa E, Sawhney V, Lanoy R, Haller N, Powell A, et al. Widespread metastases after resection of noninvasive thymoma. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2008; 26(10): 1752-5. doi: 10.1200/ jco.2007.14.5656.
- Ruffini E, Mancuso M, Oliaro A, Casadio C, et al. Recurrence of thymoma: Analysis of clinicopathologic features, treatment, and outcome. The Journal of thoracic and cardiovascular surgery. 1997; 113(1): 55-63. doi: 10.1016/s0022-5223(97)70399-4.
- Kondo K, Monden Y. Lymphogenous and hematogenous metastasis of thymic epithelial tumors. The Annals of thoracic surgery. 2003; 76(6): 1859-64. doi: 10.1016/s0003-4975(03)01017-8.