
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A case of C-ANCA positive pauci- immune crescentic glomerulonephritis not responding to corticosteroids, cyclophosphamide and rituximab: The need for novel targeted therapy!
Khin Phyu Pyar1*; Moe Zaw Myint2; Kyaw Zaw Lin3; Win Kyaw Shwe4; Aung Zaw Htet5; Myat Ko Ko6; Aung Nyan Lynn2; Moe Htun Zaw5; Kyaw Thu Yein Lwin5; Lay Maung Maung5; Ye Min Hein5; Lynn Htet Aung5; Sai Aik Hla5; Min Aung Hein5; Chan Pyae Aung5; Myo Min Thant5; Htun Htun Oo6; Myat Kyaw6; Nyein Chan Ko6; Tun Linn Kyaw6; Aung Kyaw Khine6; Zin Phyo Hlaing7; Sai Su Phone8; Min Lynn Zaw Oo8
1Professor and Head/Senior Consultant Physician and Nephrologist, Department of Medicine/Nephrology, Defence Services Medical Academy/No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
2Senior Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
3Consultant Nephrologist, Department of Nephrology, No. (1) Military Hospital (700-Bedded), Pyin Oo Lwin, Myanmar.
4Consultant Nephrologist, Department of Nephrology, No. (2) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
5Consultant Nephrologist, Department of Nephrology, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
6Nephrology Fellow, Department of Nephrology, Defense Services Medical Academy, Yangon, Myanmar.
7Consultant Pathologist, Department of Pathology, Defense Services Medical Academy, Yangon, Myanmar.
8Consultant Rheumatologist, Department of Rheumatology, General Hospital (1,000-Bedded), Nay Pyi Taw, Myanmar.
*Corresponding Author : Khin Phyu Pyar
Professor and Head/Senior Consultant Physician
and Nephrologist, Department of Medicine/
Nephrology, Defence Services Medical Academy/
No. (1) Defence Services General Hospital
(1000-Bedded), Yangon, Myanmar.
Email: khinphyupyar@gmail.com
Received : Jan 04, 2025
Accepted : Jan 28, 2025
Published : Feb 04, 2025
Archived : www.jcimcr.org
Copyright : © Pyar KP (2025).
Abstract
A 32-year-old man presented with hypertension and high serum creatinine. He had impaired hearing, sneezing, erythematous rash over leg, episcleritis, myalgia and polyarthritis for one month. Renal biopsy revealed pauci-immune crescentic glomerulonephritis; blood for c-ANCA was positive. He was given aggressive immunosuppressive treatment with corticosteroids, cyclophosphamide and rituximab. Rescue renal replacement therapy (hemodialysis) was initiated as serum creatinine was rising. However, he was on maintenance hemodialysis till now; he had oliguria, refractory hypertension requiring 5 anti-hypertensive drugs.
Keywords: C-ANCA; Pauci-immune crescentic glomerulonephritis; Aggressive immunosuppressive treatment.
Citation: Pyar KP, Myint MZ, Lin KZ, Shwe WK, Htet AZ, et al. A case of C-ANCA positive pauci- immune crescentic glomerulonephritis not responding to corticosteroids, cyclophosphamide and rituximab: The need for novel targeted therapy!. J Clin Images Med Case Rep. 2025; 6(2): 3453.
Introduction
Nephritic syndrome includes hypertension, oedema and raised serum creatinine; hematuria may exist. It is a clinical syndrome due to several etiologies: infective, inflammatory/autoimmune or malignancy. Renal histology is essential for diagnosis, treatment and prognosis particularly in adults [1].
Crescentic Glomerulonephritis (GN) is a histopathologic diagnosis characterized by extracapillary proliferation involving more than 50% of glomeruli. Clinically crescentic GN is characterized by a nephritic syndrome rapidly progressing to End Stage Renal Disease (ESRD).
Three types of crescentic GN have been identified. ‘Type 1’ includes cases of Goodpasture syndrome characterized by linear deposits of antibodies along the Glomerular Basement Membrane (GBM) at immunofluorescence. ‘Type 2’ is a heterogeneous group of primary or secondary glomerular diseases complicated by crescentic GN; granular deposits of im- munoglobulins and complement fractions on the glomerular tuft. ‘Type 3’ includes cases of ANCA-associated small-vessel vasculitis; immunofluorescence is negative or may show only faint deposits of immunoglobulins. The etiology and the initial pathogenetic factors are different in the three types of crescentic GN; however, the final mechanisms leading to crescent formation are similar. And, all 3 types have same the renal symptoms and signs. Rapidly Progressive Glomerulonephritis (RPGN) is a clinical and pathological syndrome; it is a term used to describe the followings: [1] rapid loss of renal function over a very short period (days to weeks); [2] nephritic urine analysis such as proteinuria, micro or macroscopic hematuria, dysmorphic Red Blood Cells (RBC), RBC casts; and [3] histopathological characteristic on renal biopsy finding like cellular crescent formation in the glomeruli which is proliferative cellular response seen outside the glomerular tuft within Bowman’s capsule having crescentic shape. Therefore, it is named as crescentic glomerulonephritis. RPGN is broadly classified based on the histo- pathology and immune complex deposition: [1] linear antibody deposition; [2] granular immune complex deposition disorders; and [3] pauci-immune (absence of deposition) disorders. Nonetheless, mixed as well as idiopathic variants were also reported [2]. Early diagnosis of crescentic GN or Rapidly Progressive Glomerulonephritis (RPGN) is extremely important for diagnosis and management in order to prevent further renal function loss [1]. Management is mainly with aggressive immunosuppressive therapy. Both successful outcome and failure were reported in several studies. Newer therapies were recommended in some reports [3] (Crescentic Glomerulonephritis: Pathogenesis and Therapeutic Potential of Human Amniotic Stem Cells, n.d.) [4,5]. Here, we made early diagnosis and aggressive immunosuppressive therapy in this case; however, his renal function did not recover.
Case presentation
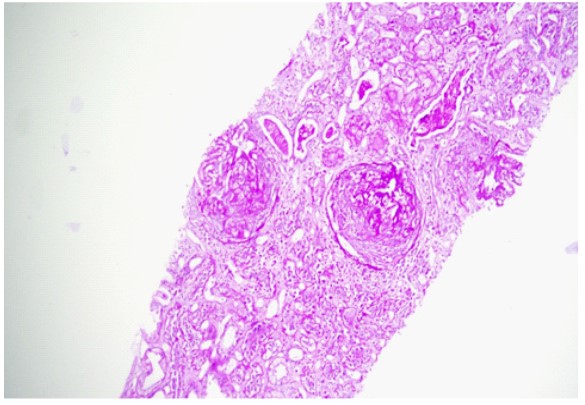
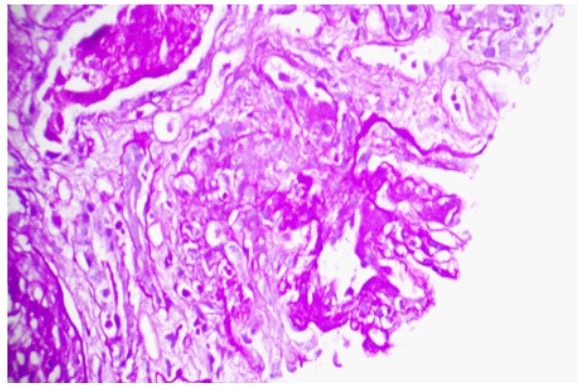
The patient was a 32 years old doctor; he was previously healthy till September 2023. He had sneezing, impaired hearing and epistaxis for 1 week duration; and, he was treated as a case of acute suppurative otitis media. He was given co-amoxiclav 625 mg 3 times a day for 10 days and topical nasal steroid spray. It was followed by episcleritis of left eye, myalgia and polyarthritis involving large joints: both knee joints, elbow joints, wrist joints and shoulder joints. They were swollen; very tender; non-migratory in nature; and, disturbing sleep even with diclofenac 50 mg 3 times a day. Initial clinical impression was acute polyarthritis due to virus (Chikungunya virus infection) or bacterial (acute rheumatic fever) in etiology. Blood for complete picture showed normal total WBC count, hemoglobin and platelet count. Inflammatory markers were raised; ESR was 10 mm in 1st hour; CRP was 6.7 mg/L; ASO titer was 200 units; serum creatinine was normal (0.93 mg/dl); uric acid was 7.4 mg/ dl. Anti-CCP was negative and RA test was positive. As RA test was positive; the likelihood of seropositive rheumatoid arthritis (RA) was also considered though several points were against it. Negative points against RA were male sex, relatively short duration of joint symptoms (less than 2 weeks), involvement of large joints. Rheumatologist suggested to start steroids, methotrexate, calcium supplements for possible seropositive rheumatoid arthritis and allopurinol for hyperuricemia. One month later, erythematous tender maculo-papular rash appeared on both shin, foot, chest and bilateral poly-chondritis developed. It is shown in photo [1-6]. Episcleritis improved though myalgia and polyarthritis were worsening. Then, he had puffy face; serum creatinine suddenly rose to 7.2 mg/dl. Blood ANA was negative. Features were highly suggestive of acute kidney injury due to acute interstitial nephritis or analgesic nephropathy. His urine output was normal. Meanwhile, he was having low grade fever. Full blood count showed normal; total WBC count was upper normal limit (12.0x109/L); hemoglobin was 12.9 gm/dl; platelet count was 406x109/L. Inflammatory markers were rising rapidly; ESR became high (70 mm in 1st hour); CRP rose to 89 mg/L. Uric acid remained high 8.2 mg/dl; liver function tests were normal; and random blood sugar was 103 mg/dl. Blood urea was very high 142 mg/dl; and, serum creatinine was very high too (8.2 mg/dl); serum potassium was 5.58 meq/L. Chest radiograph was normal. It is revealed in photo [7]. Ultrasound kidney was suggestive of bilateral mild nephropathy. In ANCA testing, p-ANCA was negative and c-ANCA was positive. Both antiproteinase 3 antibody and anti-myeloperoxidase antibody were negative. Renal biopsy was done. The features were suggestive of a pauci- immune crescentic glomerulonephritis; all glomeruli showed circumferential cellular crescents; the underlying glomerular tufts showed no increase cellularity; no basement membrane thickening; no segmental lesion; tubular injury with flattening; denudation of lining epithelium of tubules; some tubules had PAS positive hyaline casts within; no significant tubular atrophy; the interstitium appeared oedematous with no fibrosis or significant inflammation; no evidence of vasculitis. In immunofluorescence staining, all were negative: no immune deposits; IgG negative; IgM negative; IgA negative; C3 negative; C1q negative; Kappa negative; and Lambda negative. There was ‘7/7 ‘cellular crescents with underlying tufts showing no increase in cellularity. It is illustrated in photo [8,9]. He was given aggressive treatment to save kidney with rituximab, methylprednisolone and cyclophosphamide. Nonetheless, his urine output was falling; serum creatinine was rising; and, features of fluid overload set in. Therefore, rescue hemodialysis was initiated after fourth dose of rituximab. However, the patient suffered dyspnoea at rest at the day after last (third) dose of intravenous cyclophosphamide. He continued to have orthopnea, falling SaO2 even after removal of fluids with hemodialysis. Therefore, high flow oxygen was initiated. He was treated as a case of ARDS with Continuous Positive Airway Pressure (CPAP); and, he recovered over one month. Ultrasonogram done 2 months later revealed bilateral nephropathy; the size of right kidney was 10.6 cm; left kidney was 11 cm; cortical echo was increased; cortico-medullary junction was blurred; no stones nor hydronephrosis; and trace amount of ascites was seen in pelvic cavity. Therefore, he continued maintenance hemodialysis; and, he was waiting for living donor kidney transplant. As he required 5 anti-hypertensive drugs to keep blood pressure at 150/90 mmHg, renal doppler was done to exclude renal artery stenosis; it was normal. And renal angiogram did not reveal stenosis or aneurysm. His medications were Atorvastatin, Ranitidine, Carvedilol 25 mg BD, Nifedipine Retard 40 mg TDS, Aldactone 25 mg OD, Telmisartan 80 mg HS, Hydralazine 25 mg QID, Duracard 8 mg BD, Callog 1 OD, Medixon 4 mg OD, S/C Erythropoietin 4000IU 3 times/ week, Selvelamer 400 mg TDS, Ferrium XT 1 OD. He has been on maintainance hemodialysis 3 times per week till now.






Discussion
The role of renal histology in patient with nephritic syndrome was pointed out in several studies; and they highlighted the importance of early aggressive treatment to salvage renal function [6]. This patient had early renal histological diagnosis, crescentic GN. Then, this patient was treated with rituximab, corticosteroids and cyclophosphamide according to guideline [7]; however, his renal function deteriorated rapidly over one month. ANCA-associated systemic vasculitis typically affects the small arteries, arterioles, and venules; and, clinical signs include skin ulcers, neuropathy, nephropathy and granulomatous lesions of eyes, sinuses, nose, throat, and lungs, known as Wegener’s granulomatosis. This patient had positive testing for c-ANCA; and, ANCA profile was negative for both antiproteinase 3 anti-body (PR3-ANCA) and an anti-myeloperoxidase antibody. According to ‘The American College of Rheumatology’; the specificity and sensitivity in the diagnosis of Wegener’s Granulomatosis (WG) with c-ANCA positivity was 96% and 92% respectively. Having upper respiratory symptoms and renal manifestation with positive ANCA with a cytoplasmic pattern in this patient was strongly suggestive of WG. Being low-income country, the exact titer of c-ANCA could not be done. Although c-ANCA is an important test for the diagnosis of WG and monitoring of the regression [8,9], we cannot monitor the progress of disease with its titer. Rituximab was reported as a well-tolerated and effective remission induction agent for severe refractory cases of WG [10]. Full remission rates was achieved in 75% of patients with ANCA-positive vasculitis refractory to treatment treated with rituximab [10-12]. Furthermore, the remission rate was also good in non-refractory cases of WG [10]. Nonetheless, in this patient, renal function deteriorated rapidly over one month even after initiation of rituximab, corticosteroids and cyclophosphamide. This case was severe form of WG requiring more potent newer therapy. This case supported the suggestion by Syed et al. ‘the requirement for newer therapy in WG’ [5,6,3]. It is one reason for case reporting. The average duration to get clinical remission after immunosuppressive therapy in refractory case of WG was reported as 2-6 months [11]. This patient received rituximab 6 doses and cyclophosphamide 8 months ago; he was on corticosteroids. However, he required maintenance hemodialysis for persistently high serum creatinine, oliguria and refractory hypertension. The action of rituximab usually start at 2 to 6 months [11]. The patient had no evi- dence of renal recovery till 8 months after rituximab. Ultrasonogram done 8 months after immunosuppressive treatment showed increased cortical echo with blurred cortico-medullary junction. In fact, this patient had RPGN, the outcome of crescentic GN; he had End Stage Renal Disease (ESRD). Chronic Kidney Disease (CKD) leads to significant morbidity and mortality worldwide; therefore, CKD should be prevented by all means. Glomerulonephritis (GN) is the second leading cause of CKD resulting in end stage renal failure. The most severe and rapidly progressive type of GN is characterized by glomerular crescent formation. This patient had crescentic GN. The current therapies for crescentic GN, which consist of broad immunosuppressive drugs, were reported as partially effective; they were non- specific. They were toxic and had many serious side effects including infections, cancer, and cardiovascular problems. Therefore, new and safer therapies were needed [14]. Selective immunosuppressive ability and safety profile of human amniotic epithelial cells (stem cells) in patients with crescentic GN should be tried (Crescentic Glomerulonephritis: Pathogenesis and Therapeutic Potential of Human Amniotic Stem Cells, n.d.) [5,15]. The renal histology of this patient was crescentic GN; this patient had received 6 doses of rituximab and corticosteroids and cyclophosphamide. Therefore, this case highlighted the need for novel targeted therapies in treatment of crescentic GN. According to Moroni & Ponticelli, the prognosis of crescentic GN depends on the timeline of diagnosis and treatment. They found that some patients requiring rescue dialysis recovered with a good renal function; however, the outcome was poor in those with very high serum creatinine at presentation [16]. Early initiation of treatment probably resulted in a complete or partial remission in most of the patients. This patient had very high serum creatinine on referral to nephrology unit. High-dose corticosteroids, cyclophosphamide and rituximab were initiated immediately after getting histology report. This patient required rescue dialysis although he received immunosuppressive therapy early. Later, this patient was on maintenance hemodialysis as a result of rapidly progressive glomerulo- nephritis [17]. Therefore, this is another reason for case reporting. The spectrum and outcomes of crescentic glomerulonephritis among 8645 kidney biopsies was studied in South India over a period of 10 years. Crescentic glomerulonephritis was rare; it was found in 200 (2.31%) of them [18]. Patients were categorized into three etiological groups in their analysis: anti-glomerular basement membrane (type I), immune complex (type II), and pauci-immune (type III). Type II was the most common (96, 46.5%), followed by type III (73, 38%) and type I (31, 15.5%). Among type III, anti-neutrophil cytoplasmic antibodies (ANCA)-associated vasculitis was seen only in ~50% of patients. Nearly one third of patients with type I were also positive for ANCA making them ‘double positive’ (Alexander, 2020). This patient was c-ANCA positive pauci-immune crescentic glomerulonephritis, very rare case. This is one reason for case sharing. This patient had c-ANCA positive pauci-immune crescentic glomerulonephritis. ANCA associated GN was relatively common in age over fifty [19]; nonetheless, this patient was early thirty. Having RPGN in unusual age is one reason for case reporting. Simsek encouraged aggressive therapy in RPGN because it was associated with serious poor prognostic factors [20,21] (Diagnostic and Therapeutic Approach in ANCA-Associated Glomerulonephritis: A Review on Management Strategies, n.d.). Kidney survival generally depended on renal histology [22]. Moreover, the specific treatment was determined by histological findings [23]. This patient had several evidences of ongoing renal damage such as oliguria; daily urine output 200 cc; refractory hypertension requiring 5 anti-hypertensive drugs; and, maintenance hemodialysis 3 times a week. Alexander et al found that presence of oliguria/anuria and increasing percentage of crescents in renal biopsy were significant predictors of end stage kidney disease [1,18]. Therefore, this patient scenario supported South India cohort study. They reported that renal survival was significantly worse in type I/III compared to type II. Types I/III, moderate to severe interstitial fibrosis and tubular atrophy, presence of oliguria/anuria and increasing percentage of crescents in renal biopsy were significant predictors of end stage kidney disease in their cohort [18]. Histology of this patient did not reveal chronicity; interstitial inflammation without fibrosis; tubular injury without atrophy; circumferential cellular crescent in 7/7 glomeruli. Nonetheless, his renal function did not recover with timely aggressive therapy. Therefore, we need newer therapy. New therapeutic targets might improve outcomes and prognosis of patients with ANCA-associated vasculitis [4,24]. Pauci-immune glomerulonephritis is another common cause of crescen- tic glomerulonephritis. It stands for the paucity of glomerular immunoglobulin deposits in renal biopsies of patients with RPGN. In immunofluorescence staining, there was no immunoglobulin deposits (IgG, IgA and IgM) in glomerulus. Xiao et al. pointed out that immune deposition may indicate lower complement C3, more severe hematuria and glomerular lesions, milder tubular atrophy, and interstitial fibrosis; however, it cannot predict the renal outcome [25]. This patient did not have immune deposit in glomeruli. Anders et al reported that most patients with pauci-immune crescentic glomerulonephritis developed pauci-immune RPGN as a manifestation of either c- or p-ANCA-associated vasculitis [23]. The study done in Africa included nearly 1,000 renal biopsies; less than 2% showed crescentic glomerulonephritis. They reported that poor outcomes were found in children who came late. This patient did not come late; his course of disease was rapidly progressive [26]. The factors responsible for a poor renal prognosis in their study were oligoanuria, high creatinine level upon admission, use of hemodialysis, and evidence of fibro-cellular and fibrous crescents.
Conclusion
Early histopathological diagnosis and timely aggressive therapy is required in cases presented with nephritic syndrome. Restoration of renal function may be achieved with aggressive immunosuppressive therapy in crescentic glomerulonephritis. Newer better safer therapy is required for treatment of crescentic glomerulonephritis to prevent end stage renal disease.
Declarations
Acknowledgment: We are thankful to Professor Ko Ko Lwin, Professor Kyaw Zay Ya, Directorate of Medical Services; Professor Myint Zaw, Professor Myo Thant for their administrative support & Professor Tin Moe Mya for laboratory support. We are also grateful to all health care personnel giving care to this patient.
Ethical consideration: Informed consent was taken from patient.
Conflict of interest: There was no COI.
Funding: No funding was obtained.
References
- Alexander SY. Crescentic glomerulonephritis: What?s different in South Asia? A single center observational cohort study [version 1; peer review: 2 approved]. In Wellcome Open Research. 2020; 5(164). https://wellcomeopenresearch.org/articles/5-164/v1
- Almaani S, Fussner LA, Brodsky S, Meara AS, Jayne D. ANCA-Associated Vasculitis: An Update. Journal of Clinical Medicine. 2021; 10(7). https://doi.org/10.3390/jcm10071446.
- Anders HJ. Diagnosis and Management of Crescentic Glomerulonephritis: State of the Art. Saudi Journal of Kidney Diseases and Transplantation. 2000; 11(3). https://journals.lww.com/ sjkd/fulltext/2000/11030/diagnosis_and_management_of_ crescentic.8.aspx.
- Andreiana I, Stancu S, Avram A, Taran L, Mircescu G. ANCA positive crescentic glomerulonephritis outcome in a Central East European cohort: A retrospective study. BMC Nephrology. 2015; 16(1): 90. https://doi.org/10.1186/s12882-015-0091-8.
- Bonek K, Brożek-Mądry E, Wroński J, Płaza M, Zielińska A, et al. Combination Treatment of Locoregionally Aggressive Granulomatosis with Polyangiitis and Cranial Base Infiltration. Brain Sciences. 2023; 13(8). https://doi.org/10.3390/brainsci13081140.
- Choi SE, Lee SB, Pyo JY, Ahn SS, Song JJ, et al. Renal histopathological predictors of end-stage kidney disease in ANCA-associated vasculitis with glomerulonephritis: A single-centre study in Korea. Scientific Reports. 2023; 13(1): 14850. https://doi. org/10.1038/s41598-023-41811-0.
- Crescentic glomerulonephritis in children: A retrospective review of data from Chris Hani Baragwanath Academic Hospital. South African Journal of Child Health. 2023; 17(1): 4-8. https:// doi.org/10.7196/SAJCH.2023.v17i1.1885.
- Crescentic Glomerulonephritis: Pathogenesis and Therapeutic Potential of Human Amniotic Stem Cells. (n.d.).
- Diagnostic and Therapeutic Approach in ANCA-Associated Glomerulonephritis: A Review on Management Strategies. (n.d.)
- Dolch M, Irlbeck M, Wessely M, Rau S, Frey L, et al. acute respiratory distress syndrome (ARDS) as primary manifestation in ANCA-associated vasculitis. In La Presse Médicale. 2013; 42(753). https://doi.org/10.1016/j.lpm.2013.02.237.
- Floege J, Jayne DRW, Sanders JSF, Tesar V, Rovin BH. KDIGO 2024 Clinical Practice Guideline for the Management of Antineutrophil Cytoplasmic Antibody (ANCA)–Associated Vasculitis. Kidney International. 2024; 105(3): 71-116. https://doi.org/10.1016/j. kint.2023.10.008.
- Jennette JC, Nachman PH. ANCA Glomerulonephritis and Vasculitis. Clinical Journal of the American Society of Nephrology: CJASN. 2017; 12(10): 1680-1691. https://doi.org/10.2215/ CJN.02500317.
- Keogh KA, Ytterberg SR, Fervenza FC, Carlson KA, Schroeder DR, et al. Rituximab for refractory Wegener’s granulomatosis: Report of a prospective, open-label pilot trial. American Journal of Respiratory and Critical Care Medicine. 2006; 173(2): 180-187. https://doi.org/10.1164/rccm.200507-1144OC.
- Kronbichler A, Bajema IM, Bruchfeld A, Mastroianni Kirsztajn G, Stone JH. Diagnosis and management of ANCA-associated vasculitis. The Lancet. 2024; 403(10427): 683-698. https://doi. org/10.1016/S0140-6736(23)01736-1.
- Moroni G, & Ponticelli C. Rapidly progressive crescentic glomerulonephritis: Early treatment is a must. Autoimmunity Reviews. 2014; 13(7): 723-729. https://doi.org/10.1016/j.autrev.2014.02.007.
- Muhammad A, Xiao Z, Lin W, Zhang Y, Meng T, et al. Acute interstitial nephritis caused by ANCA-associated vasculitis: A case-based review. Clinical Rheumatology. 2024; 43(3): 1227-1244. https://doi.org/10.1007/s10067-023-06798-z.
- Naik RH, Shawar SH. Rapidly Progressive Glomerulonephritis (32491362). StatPearls Publishing, Treasure Island (FL); PubMed 2023. http://europepmc.org/abstract/MED/32491362.
- Pallan L, Savage CO, Harper L. ANCA-associated vasculitis: From bench research to novel treatments. Nature Reviews Nephrology. 2009; 5(5): 278-286. https://doi.org/10.1038/nrneph.2009.45.
- Powers B, Uppalapati A, Gogineni S, Jamkhana ZA. Rituximab-a drug with many facets and cures: A treatment for acute refractory hypoxemic respiratory failure secondary to severe granulomatosis with polyangiitis. Case Reports in Critical Care. 2013; 123134. https://doi.org/10.1155/2013/123134.
- Renson T, Kelly MM, Benediktsson H, Grundhoefer N, Luca N, et al. Non-invasive biomarkers of disease activity and organ damage in ANCA-associated vasculitis: A systematic review. RMD Open. 2024; 10(1): 003579. https://doi.org/10.1136/rmdopen-2023-003579.
- Rowaiye OO, Kusztal M, Klinger M. The kidneys and ANCA-associated vasculitis: From pathogenesis to diagnosis. Clinical Kidney Journal. 2015; 8(3): 343-350. https://doi.org/10.1093/ckj/ sfv020.
- Simsek B. A stagerring recovery of an adolescent boy with crescentic glomerulonephritis despite numerous poor prognostic factors following early therapy. In J Renal Inj Prev. 2024; 13(3): 34302-34302.
- Syed R, Rehman A, Valecha G, El-Sayegh S. Pauci-Immune Crescentic Glomerulonephritis: An ANCA-Associated Vasculitis. BioMed Research International, 2015; 402826. https://doi. org/10.1155/2015/402826.
- Tansakul E, Srisuwarn P. ANCA-associated Glomerulonephritis. Journal of the Nephrology Society of Thailand. 2023; 29(3): 154-165.
- Wu T, Peng J, Meng T, Liu Q, Ao X, et al. Clinicopathological features and prognostic analysis of 49 cases with crescentic glomerulonephritis. Experimental and Therapeutic Medicine. 2019; 18(5): 3984-3990. https://doi.org/10.3892/etm.2019.8023.
- Xiao X, Ren H, Gao P, Yin D, Li C, et al. What is the prognosis of ANCA-associated glomerulonephritis with immune deposition? Renal Failure. 2022; 44(1): 1478-1486. https://doi.org/10.1080/ 0886022X.2022.2114368.