
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Chronic rectal bleeding in young adults: Exploring the rare diagnosis of rectal vascular malformation
Marques C*; Ferreira C; Vaz Pereira R; Leal C; Vieira B; Pinto-de-Sousa J
CACTMAD - Centro Académico Clínico de Trás-os-Montes e Alto Douro, Av. da Noruega, Lordelo 5000-508 Vila Real, Portugal.
*Corresponding Author : Carolina Marques
CACTMAD - Centro Académico Clínico de Trás-os-
Montes e Alto Douro, Av. da Noruega, Lordelo 5000508 Vila Real, Portugal.
Email: carolina9marques@gmail.com
Received : Jan 06, 2025
Accepted : Jan 29, 2025
Published : Feb 05, 2025
Archived : www.jcimcr.org
Copyright : © Marques C (2025).
Citation: Marques C, Ferreira C, Pereira RV, Leal C, Vieira B, et al. Chronic rectal bleeding in young adults: Exploring the rare diagnosis of rectal vascular malformation. J Clin Images Med Case Rep. 2025; 6(2): 3454.
Description
Rectal Vascular Malformations (RVM) are rare and poorly documented, primarily relying on case reports and a small number of case studies found in the literature [1-4]. Typically, this condition leads to painless rectal bleeding in young adults, with more than half of the cases presenting with anemia [2,5,6]. Additional symptoms, such as constipation and abdominal pain, have also been documented [3] and 10% of the cases are incidentally diagnosed [3,5].
Since the physical examination, including digital rectal examination, can be inconclusive, there are various complementary diagnostic methods that assist in the diagnosis and management of this pathology, such as colonoscopy, contrast-enhanced Computerized Tomography (CT) scan, and Magnetic Resonance Imaging (MRI) [6-8].
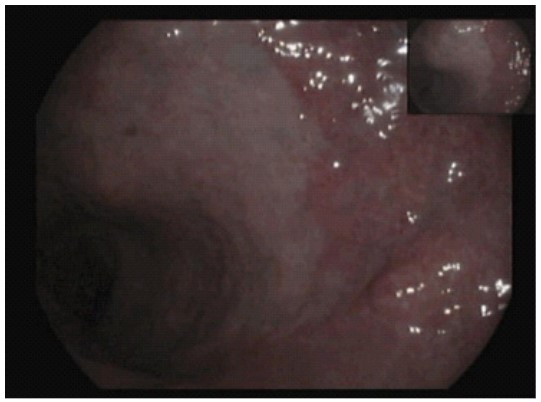
Colonoscopy is a valuable tool for diagnosis and determining the extent of the disease. The presence of multiple bluish-purple submucosal masses, indicative of dilated tortuous blood vessels, strongly suggests vascular malformation (VM) [3,4,9,10].
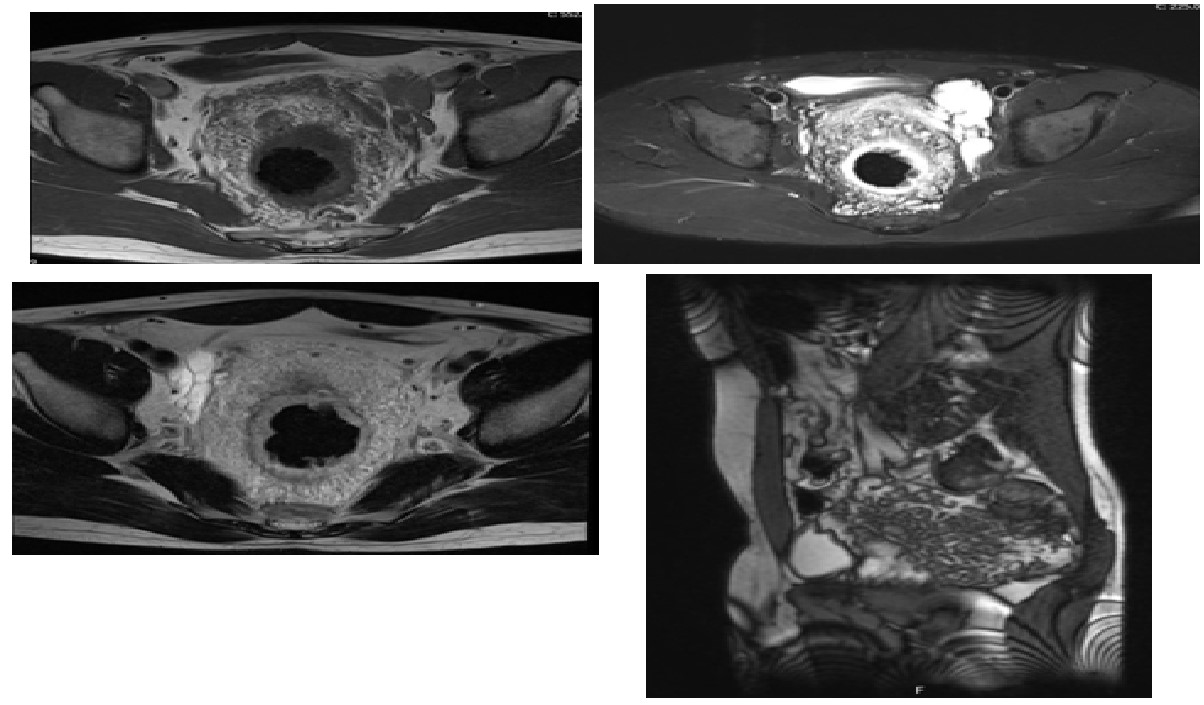
CT angiography aids in characterizing the disease, outlining its extent, and assessing involvement with adjacent structures [9]. Moreover, CT angiography can identify the vascular supply of high-flow lesions, reveal draining vessels, and indicate the presence of phleboliths, characteristic of low-flow venous malformation. However, for VM-related lesions, especially in follow-up, MRI outperforms CT. On T2-weighted images, MRI enables the detection of high-signal-intensity wall thickening with multiple serpiginous structures in the perirectal region, suggesting increased vascularity and blooming phleboliths. MRI is also superior to CT in locating the upper limit of the lesion and assessing its extension into adjacent organs [9].
A biopsy of these lesions is not recommended due to the risk of severe bleeding [11].
We present the case of a 49-year-old man referred to a general surgery consultation due to chronic anal pain since childhood and episodes of rectal bleeding persisting for 17 years. Additionally, he was being monitored in hematology due to an iron-deficiency anemia and was receiving optimized medical treatment. There were no alterations to the physical examination.
He performed a colonoscopy (Figure 1), CT scan (Figure 2), and MRI (Figure 3).
The treatments described for this pathology are abdominoperineal resection or anterior rectum resection with total mesorectal excision. Vascular embolization, radiotherapy and sclerotherapy have been suggested as management options, but they have had varying degrees of success. These conservative therapies are limited to poor candidates for surgical resection due to RVM´s transmural involvement and risk of recurrence [10].
The case was discussed in a multidisciplinary team, including vascular and general surgeons and the advantages and risks of the surgery were explained to the patient. Since the symptoms have been controlled lately, the patient refused the surgery, keeping follow-up in the consultation.

References
- Bhattacharjee HK, Nariampalli Karthyarth M, Suhani S, Goyal A, Das NR, Sharma R, et al. Laparoscopic total mesorectal excision for rectal venous malformation: A case report with a brief literature review. Asian J Endosc Surg. 2021; 14: 85–9.
- Sylla P, Deutsch G, Luo J, Recavarren C, Kim S, Heimann TM, et al. Cavernous, arteriovenous, and mixed hemangioma–lymphangioma of the rectosigmoid: rare causes of rectal bleeding—case series and review of the literature. Int J Colorectal Dis. 2008; 23: 653–8.
- Hervías D, Turrión JP, Herrera M, Navajas León J, Pajares Villarroya R, Manceñido N, et al. Diffuse cavernous hemangioma of the rectum: an atypical cause of rectal bleeding. Rev Española Enfermedades Dig. 2004; 96.
- Fujikawa H, Araki T, Hashimoto K, Okita Y, Tanaka K, Hiro J, et al. Sphincter-Saving Resection of Rectal Hemangioma Based on Doppler Transrectal Ultrasonography Findings: Report of a Case. Int Surg. 2014; 99: 705–9.
- Wang HT, Gao XH, Fu CG, Wang L, Meng RG, Liu LJ. Diagnosis and Treatment of Diffuse Cavernous Hemangioma of the Rectum: Report of 17 Cases. World J Surg. 2010; 34: 2477–86.
- Wang H, Gao Y. Diffuse cavernous hemangioma of the rectum: case report and literature review. Int J Colorectal Dis. 2016; 31: 1067–8.
- Parashette KR, Cuffari C. Sclerotherapy of Rectal Hemangiomas in a Child with Klippel-Trenaunay-Weber Syndrome. J Pediatr Gastroenterol Nutr. 2011; 52: 111–2.
- Wilson CL, Wong Kee Song L-M, Chua H, Ferrara M, Devine RM, Dozois RR, et al. Bleeding from cavernous angiomatosis of the rectum in Klippel-Trenaunay syndrome: report of three cases and literature review. Am J Gastroenterol. 2001; 96: 2783–8.
- Zuccaro G. Management of the Adult Patient with Acute Lower Gastrointestinal Bleeding. Am J Gastroenterol. 1998; 93: 1202–8.
- Vitor S, Oliveira Ferreira A, Lopes J, Velosa J. Hemangioma of the rectum - How misleading can hematochezia be? Rev Esp enfermedades Dig. 2016; 108: 500–1.
- Abeysekera KWM, Pearl DS, Burn P, Lowe A. Incidental finding of diffuse cavernous rectal haemangiomatosis during bowel cancer screening. BMC Gastroenterol. 2019; 19: 198.