
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 6
Acute disseminated encephalomyelitis following bacterial meningoencephalitis: Two case reports & review of literature
Megha Priyadarshi1; Ayush Mohan2; Pranjal Gupta2; Vinay Goel3; Ayush Agarwal2; Satish Barki4; Rohit Bhatia2; Manish Salunkhe5*
1Department of Infectious Diseases, All India Institute of Medical Sciences, India.
2Department of Neurology, All India Institute of Medical Sciences, India.
3Department of Neuroradiology & Radiodiagnosis and Interventional Radiology, All India Institute of Medical Sciences, India.
4Department of Neurology, Army Hospital Research & Referral, India.
5Associate Consultant, Department of Neurology, Nanavati Max Super-Speciality Hospital, India.
*Corresponding Author : Manish Salunkhe
Associate Consultant, Department of Neurology,
Nanavati Max Super-speciality Hospital, Mumbai,
India.
Tel: 9834703694
Email: manishsalunkhe132@gmail.com
Received : Jan 08, 2025
Accepted : Jan 29, 2025
Published : Feb 05, 2025
Archived : www.jcimcr.org
Copyright : © Salunkhe M (2025).
Abstract
Acute Disseminated Encephalomyelitis (ADEM) is commonly associated with viral infections, but its occurrence after bacterial meningoencephalitis is rare. This study presents a case of ADEM following bacterial meningoencephalitis and reviews related case reports. A literature search was performed using PubMed and EMBASE to identify case reports of ADEM post-bacterial meningoencephalitis. A 37-year-old woman developed right hemiparesis and encephalopathy after recovering from pyogenic meningitis. Brain MRI revealed multiple T2/FLAIR lesions consistent with post-infective ADEM. Treatment with steroids and plasma exchange resulted in significant improvement, and she remained asymptomatic after one year. A 37-year-old woman presented with meningitis and improved with antibiotics. However, she later developed right-sided weakness and encephalopathy. Brain MRI showed multifocal T2/FLAIR lesions, and post-infective ADEM was diagnosed. She improved significantly after treatment with intravenous steroids, with full resolution of symptoms after seven months. Eleven cases were reviewed, with a median patient age of 41 years. Focal deficits were common, reported in 81.8% of cases. Multifocal cerebral lesions were present in all patients, and 90.9% had neutrophilic pleocytosis. Causative bacteria were identified in 81.8% of cases, with clinical improvement in 90.9%. ADEM can develop after bacterial meningoencephalitis and should be considered in cases of neurological decline following initial improvement from the infection.
Keywords: Bacterial meningoencephalitis; Acute disseminated encephalomyelitis; Post-infectious neurological syndrome; Molecular mimicry.
Citation: Priyadarshi M, Mohan A, Gupta P, Goel V, Salunkhe M, et al. Acute disseminated encephalomyelitis following bacterial meningoencephalitis: Two case reports & review of literature. J Clin Images Med Case Rep. 2025; 6(2): 3455.
Introduction
Post-Infectious Neurological Syndromes (PINS) encompass a wide range of clinical presentations, affecting both the Central Nervous System (CNS) and Peripheral Nervous System (PNS) [1]. The association between Acute Disseminated Encephalomyelitis (ADEM) and viral infections is well-established, with 50-75% of adult ADEM cases linked to preceding viral infections [2]. However, there is limited literature regarding the association of bacterial infections with ADEM. Some bacterial pathogens, such as Mycoplasma pneumoniae, Borrelia burgdorferi, Legionella pneumoniae, and Group A beta-hemolytic streptococci, have been implicated in PINS [3].
In this report, we present two cases of patients initially diagnosed with bacterial meningitis who subsequently developed ADEM. In addition, we provide a review of the literature to further characterize this rare clinical entity of ADEM following bacterial meningitis or meningoencephalitis [4-12].
This paper aims to shed light on the under-recognized relationship between bacterial meningoencephalitis and ADEM and to emphasize the importance of considering ADEM as a differential diagnosis in patients with clinical deterioration after recovering from bacterial meningitis.
Case presentations
Case report 1
A 37-year-old woman presented with the acute onset of a holocranial headache, fever, and multiple episodes of vomiting, followed by encephalopathy over the course of 2-3 days. On examination, she was irritable, and meningeal signs were present. Brain MRI revealed mild effacement of the sulcal and cisternal spaces bilaterally (Figure 1A). Laboratory investigations at the time of admission showed the following: hemoglobin of 7.8 g/ dL, white blood cell count of 12,700/μL (85% neutrophils), and C-Reactive Protein (CRP) of 16 mg/L. Cerebrospinal Fluid (CSF) analysis revealed a white blood cell count of 1,145 cells/μL, with 90% polymorphonuclear cells, protein level of 600 mg/dL, and glucose level of 54 mg/dL (random blood sugar: 100 mg/ dL). Gram staining of the CSF showed Gram-positive cocci, and Staphylococcus aureus was cultured. Additional tests, including CSF Ziehl-Neelsen (ZN) stain, cryptococcal antigen, Indian ink preparation, CSF Tuberculosis (TB) PCR, and CSF TB GeneXpert, were negative. A diagnosis of pyogenic meningitis was made, and she was treated with antibiotics for two weeks, resulting in complete symptom resolution.
However, one week after discharge, she developed a headache and vomiting. Two days later, she experienced the acute onset of right-sided weakness (modified Rankin Scale - mRS 5) and slurred speech. Her sensorium progressively worsened. A repeat brain MRI revealed multiple T2/FLAIR hyperintense confluent lesions involving the subcortical deep and periventricular white matter of the fronto-parietal and anterior temporal lobes bilaterally (left greater than right), left basal ganglia, left insula, corpus callosum, and midbrain (Figure 1B). Repeat CSF analysis showed a white blood cell count of 2 cells/μL, protein level of 50 mg/dL, and glucose level of 115 mg/dL. Evaluation for autoimmune encephalitis, including serum Antibodies for Aquaporin-4 (AQP4) and Myelin Oligodendrocyte Glycoprotein (MOG), was negative.
Given the diagnosis of post-infective ADEM, she was treated with a 1000 mg pulse of Intravenous (IV) Methylprednisolone (MPS) for five days. This led to some improvement in her sensorium, although she had a persistent motor deficit. A repeat MRI four weeks after disease onset showed new lesions in the thalamus and left basal ganglia, an increase in the size of the frontal lobe lesions, and regression of the lesion in the left anterior temporal lobe.
Due to her partial response to steroids, she underwent five cycles of plasma exchange, after which she improved significantly, though with some residual limb weakness (mRS 1). At her one-year follow-up, she remained asymptomatic, and imaging showed complete resolution of the lesions (Figure 1C).
Case report 2
A 37-year-old woman with no prior comorbidities presented with an acute onset of headache, followed by multiple episodes of vomiting and altered sensorium within one day. On clinical examination, she was arousable to painful stimuli, with neck rigidity noted. An initial Non-Contrast CT (NCCT) of the head was normal. Cerebrospinal Fluid (CSF) analysis showed elevated cell count, with a predominance of polymorphonuclear cells, elevated protein, and reduced glucose levels. CSF Gram stain and culture were negative, as were CSF GeneXpert and TB PCR tests. The patient was started on intravenous antibiotics and was discharged after five days at her request, with a plan to continue IV antibiotics for another five days at home. She showed improvement and returned to her baseline level of functioning.
Two weeks after the initial presentation, her relatives observed slowness in her activities, along with reduced movement in her right upper and lower limbs, progressing over 2-3 days. The next day, the patient became encephalopathic and was rehospitalized. A brain MRI at this stage revealed multifocal T2/ FLAIR hyperintense lesions involving the left fronto-parietal white matter and the genu of the corpus callosum. A radiological diagnosis of post-infective ADEM or tumefactive demyelination was considered, and the patient was referred to a higher center, where she was subsequently admitted.
At our center, the patient was evaluated and found to have non-fluent aphasia, right hemiparesis, and a positive right extensor plantar reflex. Repeat CSF analysis showed a Total Leukocyte Count (TLC) of 15 cells/μL, with 33% neutrophils, protein of 82 mg/dL, and glucose of 75 mg/dL. Testing for autoimmune encephalitis antibodies, as well as serum aquaporin-4 (AQP4) and Myelin Oligodendrocyte Glycoprotein (MOG) antibodies, was negative. A repeat brain MRI demonstrated extension of the lesion into the right frontal white matter. Infective workup, including CSF Gram stain, culture, and GeneXpert, was negative.
The patient was started on pulse therapy with Intravenous Methylprednisolone (IV MPS) for five days, which led to significant improvement in her symptoms. She was subsequently discharged on oral steroids. At her seven-month follow-up, she had minimal residual symptoms and was independent in all her activities. A repeat brain MRI showed near-complete resolution of the lesion.
Methodology
Two authors independently conducted a literature review to identify cases of Acute Disseminated Encephalomyelitis (ADEM) following bacterial meningoencephalitis. The data-bases PubMed and EMBASE were searched using the following terms: PubMed: “Encephalomyelitis, Acute Disseminated” AND “Meningoencephalitis,” and “Encephalomyelitis, Acute Disseminated” AND “Meningitis, Bacterial”; EMBASE: “acute disseminated encephalomyelitis” AND “bacterial meningitis,” and “acute disseminated encephalomyelitis” AND “bacterial meningoencephalitis.” All relevant published articles were reviewed for inclusion.
We included cases that met the following criteria: A) Clinical presentation of fever and meningoencephalitis. B) Cerebrospinal Fluid (CSF) analysis demonstrating neutrophilic pleocytosis and/or evidence of bacterial infection, as confirmed by Gram stain, CSF bacterial culture, CSF PCR, or CSF antigen testing. C) Patients satisfying the International Paediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders, as revised in 2013. D) Patients aged over 14 years. E) Articles published in the English language.
A total of 153 articles were initially screened for relevance. After reviewing the cases, we identified 16 reported cases of ADEM following bacterial meningitis. Of these, two were excluded due to being written in Japanese, three were excluded due to patient age being less than 14 years, and one case was excluded because it only described radiological findings suggestive of ADEM without any clinical evidence of encephalitis. Ultimately, 11 patients, including the two cases presented in this study, were included in the final analysis.
Results
The median age of the patients was 41 years (range: 35- 61.5). Co-morbid conditions were present in 54.55% (6/11) of patients, and one patient had a history of vaccination within four weeks of symptom onset. All patients presented with fever, while 54.55% (6/11) experienced headaches, and 81.8% (9/11) had neck rigidity at the time of admission. No patient reported seizures during the course of the illness. Focal neurological deficits were observed in 81.8% (9/11) of patients. Two patients developed myelitis, and one patient had optic neuritis. None of the patients experienced a relapse during a median follow-up period of 12 months (range: 3-12 months). All patients had multifocal cerebral lesions, with 45.45% (5/11) showing infratentorial involvement. Spinal cord lesions were observed in 18.18% (2/11) of patients.
CSF neutrophilic pleocytosis was noted in 90.9% (10/11) of patients, with a median CSF white blood cell count of 635 cells/μL (range: 469-1132.5). Elevated CSF protein levels were found in 90.9% (10/11) of patients, with a median protein level of 193.5 mg/dL (range: 84.75-522.5). Bacterial pathogens were isolated in 72.7% (8/11) of cases, with CSF culture being the most common diagnostic method (45.45% [5/11]). Streptococcus pneumoniae was the most frequently identified organism (25%). None of the patients tested positive for any immunological antibodies.
All patients received Intravenous (IV) antibiotics, either empirically or based on culture sensitivity, to treat bacterial meningoencephalitis. IV Methylprednisolone (MPS) was administered to 90.9% (10/11) of patients, while one patient received oral steroids for ADEM. Only the present case was treated with plasma exchange following IV MPS therapy. None of the patients received Intravenous Immunoglobulin G (IVIG).
Clinical outcomes were reported for all patients. Improvement was observed in 90.9% (10/11) of cases. Follow-up CSF analysis was available for 72.7% (8/11) of patients, all of whom showed a reduction in CSF white blood cell counts. Follow-up MRI demonstrated a reduction in lesion size in 90.9% (10/11) of patients. One patient had an increase in lesion size and died during the course of the disease. No patients experienced a relapse of ADEM or any other demyelinating events during the median follow-up period of 12 months (range: 3-12 months).
Discussion
Acute Disseminated Encephalomyelitis (ADEM) is an inflammatory demyelinating disorder, more commonly seen in children, with a male preponderance and an incidence of 0.2–0.4 per 100,000, as reported in various nationwide studies (Otallah et al., 2021). Although ADEM is primarily associated with viral infections, bacterial and parasitic infections have also been implicated in its etiology [13]. The latency period between infection and the onset of symptoms typically ranges from two to four weeks, and clinicians should investigate other causes when the latency exceeds eight weeks [14,15]. Upper respiratory tract viral infections are the most common triggers of ADEM; however, it can also be precipitated by exanthematous illnesses or gastroenteritis. Post-bacterial meningitis ADEM is a rare occurrence, with only a few cases reported in the literature. In our case, ADEM developed after Staphylococcus aureus meningitis.
The median age of patients in our report was older than that reported for adult-onset ADEM in the literature. For example, in a study by Koelman et al., the median age for adult-onset ADEM was 37 years (range: 27–49) [16]. Another study by Marchioni et al. reported a mean age of 46.7 years for post-infectious encephalomyelitis [17].
The presence of fever and meningeal signs differentiates post-bacterial meningitis ADEM from other forms of monophasic ADEM. In the largest retrospective American cohort, 25% of adult ADEM patients had a fever, and 10% exhibited meningeal signs. In our literature review, we did not observe any gender predilection, which is consistent with findings from previous cohorts of post-infectious encephalomyelitis [16].
In the present cases, the initial clinical findings were consistent with bacterial meningitis, supported by bacterial cultures from the CSF in one case. Among the reported cases in this review, the pathogen was not identified in 3 of 11 patients. This is consistent with community-acquired meningitis, where causative organisms remain unidentified in approximately 20% of cases [4]. The median CSF cell count and protein levels in our cases were higher than those typically seen in ADEM, making viral or fungal meningitis and early presentation of ADEM less likely. The improvement in CSF findings after IV antibiotics further supports the initial diagnosis of bacterial meningitis.
In our cases, after initial improvement, both patients experienced secondary deterioration characterized by a left-hemispheric syndrome. MRI brain scans at the time of this second clinical event revealed characteristic ADEM lesions, including multifocal supratentorial and infratentorial lesions, large cortical-subcortical lesions, and involvement of deep gray nuclei, supporting the diagnosis of post-infectious ADEM.
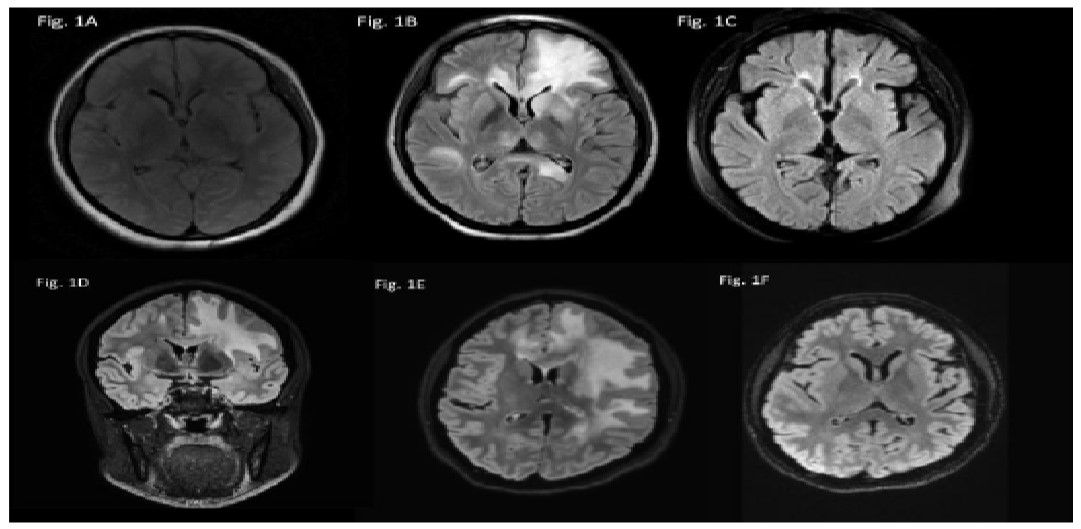
Table 1: Clinical and demographic profiles of the cases & organisms isolated in CSF.
| Publication | Sex/Age | Comorbid conditions | Fever | Headache | Meningeal signs | Focal deficits | Myelitis | Optic neuritis | Organism isolated | Method |
|---|---|---|---|---|---|---|---|---|---|---|
| 2021/Ohrrnar et al. (Case 1) | M/41 | DM, CKD, chronic active Hepatitis B | Yes | No | Yes | No | No | No | Sphingomonas paucimobilis | CSF culture |
| 2020/Niederschweiberer et al. (Case 2) | M/62 | None | Yes | No | Yes | Yes | No | No | None | NA |
| 2015\1Kato et al. (Case 3) | F/85 | COPD | Yes | No | Yes | Yes | No | No | None | NA |
| 2014/Majzoobi et al. (Case 4) | M/24 | None | Yes | No | Yes | Yes | No | No | Streptococcus pneumoniae | Gram stain, CSF culture |
| 2014/ Huhn et al. (Case 5) | F/61 | Splenectomy | Yes | Yes | Yes | Yes | No | No | Streptococcus Pneumoniae | CSF & blood culture |
| 2009/ Okada et al. (Case 6) | F/73 | Hypertension | Yes | Yes | Yes | Yes | No | No | Mycobacterium intracellulare | CSF PCR |
| 2008/Beleza et al. (Case 7) | M/17 | Glomerulopathy | Yes | Yes | Yes | No | No | No | Hemophillus influenza B | CSF antigen |
| 2004/Assen et al. (Case 8) | M/45 | None | Yes | No | No | No | Yes | Yes | Borrelia burgdorferi | CSF & Brain biopsy PCR |
| 2003/Proulx et al. (Case 9) | F/33 | None | Yes | Yes | Yes | No | No | No | Pasteurella multocida | Gram stain, CSF & blood culture |
| 2024/Pliyadarshi et al. (Case 10) | F/37 | Iron deficiency anaemia | Yes | Yes | Yes | No | No | No | Staphylococcus aureus | Gram stain, CSF culture |
| 2024/Pliyadarshi et al. (Case 11) | F/37 | None | No | Yes | Yes | No | No | None | None | Gram stain, CSF culture |
Note: DM: Diabetes Mellitus; CKD: Chronic Kidney Disease; CSF: Cerebrospinal Fluid; COPD: Chronic Obstructive Airway Disease; PCR: Polymerase Chain Reaction.
Table 2: CSF & MRI findings at the time presentation, follow up & outcome of the cases.
| Case | CSF TLC (cells/μL) | CSF protein (mg/dl) | CRP (mg/dl) | MRI findings (FLAIR hyperintensity) | Treatment received | Follow up CSF Improved? | Follow up MRI Improved? | Clinical Outcome | Total follow up (Months) |
|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 2 | 14 | NA | Multifocal cerebral | Cefepime, IV MPS | NA | Yes | Improved | 3 |
| Case 2 | 635 [PMN predominant] | 220 | NA | Multifocal cerebral | Ceftriaxone, Ampicillin, Acyclovir & IV MPS | Yes | Yes | Improved | 2.6 |
| Case 3 | 615 [P-95, M-5] | 243 | 16 | Multifocal cerebral, brainstem, cerebellum & LETM dorsal segment | Meropenem, Dexamethasone & IV MPS | Yes | Yes | Minimally improved | 1 |
| Case 4 | 610 [P-60] | 350 | NA | Multifocal cerebral & pons | Ceftriaxone, Vancomycin & Prednisolone | Yes | Yes | Improved | 3 |
| Case 5 | 5200 [Neutrophilic predominant]* | 580 | 420 | Multifocal cerebral | Penicillin G, IV MPS | Yes | Yes | Improved | 12 |
| Case 6 | 1295 [P-60, L-40] | 60 | 1.59 | Multifocal cerebral & cerebellum | Streptomycin, Rifampicin, Clarithromycin & IV MPS | Yes | Yes | Improved | 14 |
| Case 7 | 1120 [P-78, L-7, Mo-15] | 144 | 7.55 | Multifocal cerebral | Cefotaxime, Rifampicin, Gentamicin & IV MPS | Yes | Yes | Improved | 12 |
| Case 8 | 328 [Neutrophilic predominant] | 264.8 | 1.3 | Multifocal cerebral, pons, medulla & thoracic spine | Ceftriaxone, Amoxicillin, Erythromycin, Acyclovir and IV MPS | Yes | No | Death | - |
| Case 9 | 680 [P-78, L-1, Mo-21] | 93 | 2.1 | Multifocal cerebral | Cefotaxime, Vancomycin, Penicillin G & IV MPS | NA | Yes | Improved | 16 |
| Case 10 | 1145 [P-90, L-10] | 600 | 16 | Multifocal cerebral, pons | Vancomycin, Cefazolin, IV MPS & Plasma exchange therapy | Yes | Yes | Improved | 12 |
| Case 11 | 15 [P-33, L-67] | 82 | 75 | Multifocal cerebral | IV, IV MPS | NA | Yes | Improved | 7 |
Note: DM: Diabetes Mellitus; CKD: Chronic Kidney Disease; CSF: Cerebrospinal Fluid; COPD: Chronic Obstructive Airway Disease; PCR: Poly-
merase Chain Reaction.
*Differential cell counts not provided.
While the association of ADEM with viral infections is well- established, its occurrence following bacterial infections is extremely rare, with limited literature available for support [3]. The leading cause of pathogen-based autoimmunity is molecular mimicry. In this process, the antigenic similarity between bacterial pathogens and brain epitopes triggers the activation of anergic autoreactive T and B lymphocytes, resulting in CNS inflammation and demyelination. These bacterial peptides exhibit cross-reactivity with myelin autoantigens, such as Myelin Basic Protein (MBP), Myelin-Associated Oligodendrocyte Basic Protein (MOBP), Oligodendrocyte-Specific Protein (OSP), and Myelin Oligodendrocyte Glycoprotein (MOG) [18].
One example of antigenic mimicry is the similarity between N-acetyl-β-D-glucosamine on the cell wall of Streptococcus pneumoniae and neuronal lysoganglioside GM1, as demonstrated by Kirvan et al. in vitro [19]. Post-streptococcal CNS syndrome due to exotoxins inducing T cell-mediated anti-myelin autoreactivity has also been proposed as a cause of the demyelinating lesions seen in ADEM [20].
In our patient, bacterial meningitis caused by Staphylococcus aureus was followed by the development of ADEM. Staphylococcus aureus has been demonstrated in in vitro studies to possess bacterial peptides that mimic Myelin Basic Protein (MBP). Chastain et al. conducted an in vitro study to investigate the ability of bacterial MBP antigen mimics to activate CNS T cell clones and study their encephalitogenic potential. In this study, humanized mice were primed with bacterial peptide mimics from Hemophilus influenzae, Staphylococcus aureus, Mycobacterium avium, Mycobacterium tuberculosis, and Bacillus subtilis. A monophasic disease pattern was induced by all mimics, except for Mycobacterium tuberculosis and Hemophilus influenzae, with homology to MBP ranging from 20-33%. CD4 T cell infiltration was observed in the cerebellum, and the degree of infiltration correlated with disease severity [21].
Molecular mimicry is linked to two other mechanisms: bystander activation and epitope spreading [21]. Bystander activation involves the activation of costimulatory pathways and cytokine release, leading to the nonspecific self-sensitization of T cells against myelin autoantigens during active infection. Epitope spreading, a consequence of persistent infection, occurs when prolonged anti-pathogen-specific immune responses cause tissue destruction, releasing endogenous or cryptic self-epitopes, which contribute to further cytokine-induced tissue damage. These mechanisms are thought to contribute to the demyelination seen in ADEM [18,21].
In a prospective study of post-infectious central demyelination syndromes, 24.6% of patients had a relapsing disease course [17]. Relapsing ADEM has been reported in up to 10% of cases in the literature [16]. However, we did not observe any relapses in this review. Evidence supporting the use of IV Immunoglobulin (IVIg) and plasma exchange in post-infectious demyelination syndromes is limited. In a study of 112 cases of central PINS, 3 of 8 (37.5%) patients responded to IVIg, but none received plasma exchange [17]. In a study of 26 pediatric PINS cases, 30% received IVIg, and only one patient was treated with plasma exchange due to a partial response to steroids [1]. In our case, plasma exchange therapy proved to be effective.
Conclusion
Our cases, along with the literature review, expand the spectrum of adult ADEM cases. Bacterial meningoencephalitis may act as a trigger for this acute inflammatory CNS response. Clinicians should consider ADEM as a differential diagnosis in cases of deterioration following initial improvement from bacterial meningoencephalitis, as it is a treatable condition with a potentially favorable clinical outcome.
Declarations
Acknowledgement: We thank all the doctors, the nurses of the neurology department in our hospital. This study was carried out as part of the routine work with no external funding.
Ethical approval: A written informed consent was obtained from the patients. These are case reports and no approval of the AIIMS research ethics committee was required.
Financial support: No funding was received to assist with the preparation of the manuscript. The authors have no financial interests to disclose.
Disclosure: There are no competing interests related to the authors of this manuscript.
References
- Bozzola E, Spina G, Valeriani M, et al. Management of pediatric post-infectious neurological syndromes. Ital J Pediatr. 2021; 47: 1–12.
- Otallah S. Acute disseminated encephalomyelitis in children and adults: A focused review emphasizing new developments. Multiple Sclerosis Journal. 2021; 27: 1153–1160.
- Massa S, Fracchiolla A, Neglia C, et al. Update on Acute Disseminated Encephalomyelitis in Children and Adolescents. Children. 2021; 8: 280.
- Niederschweiberer J, Lauerer M, Schweyer K, et al. Acute disseminated encephalomyelitis following Tdap vaccination and bacterial meningoencephalitis. Mult Scler Relat Disord. 2020; 46.
- Kato Y, Hayashi T, Uchino A, et al. Parainfectious encephalomyeloradiculitis associated with bacterial meningitis: A case report. J Med Case Rep. 2015; 9: 10–12.
- Majzoobi MM, Mamani M, Ghiasian M, Abdoli E. Acute Disseminated Encephalomyelitis Following Pneumococcal Meningitis Infection. Avicenna Journal of Clinical Microbiology and Infection. 2014; 1: 20612–20612.
- Huhn K, Lee DH, Linker RA, et al. Pneumococcal-meningitis associated acute disseminated encephalomyelitis (ADEM) - case report of effective early immunotherapy. Springerplus. 2014; 3: 1–5.
- Okada H, Yoshioka K. Acute disseminated encephalomyelitis associated with meningitis due to Mycobacterium intracellulare. Internal Medicine. 2010; 49: 2113–2116.
- Beleza P, Ribeiro M, Pereira J, et al. Probable acute disseminated encephalomyelitis due to Haemophilus influenzae meningitis. Dev Med Child Neurol. 2008; 50: 388–391.
- van Assen S, Bosma F, Staals LME, et al. Acute disseminated encephalomyelitis associated with Borrelia burgdorferi [6]. J Neurol. 2004; 251: 626–629.
- Proulx NL, Freedman MS, Chan JW, et al. Acute disseminated encephalomyelitis associated with Pasteurella multocida meningitis. Canadian Journal of Neurological Sciences. 2003; 30: 155–158.
- Ohnmar O, Kyaw M, Lwin T.Acute disseminated encephalomyelitis due to Sphingomonas paucimobilis meningitis. Neurol Clin Neurosci. 2021; 9: 384–386.
- Paolilo RB, Deiva K, Neuteboom R, et al. Acute Disseminated Encephalomyelitis: Current Perspectives. Children. 2020; 7: 210.
- Nishiyama M, Nagase H, Tomioka K, et al. Clinical time course of pediatric acute disseminated encephalomyelitis. Brain Dev. 2019; 41: 531–537.
- Giri PP, Bhattyacharya S, Das D, Mukhopadhaya S. Acute disseminated encephalomyelitis: A clinical and neuroradiological profile of pediatric patients. Neurol India. 2016; 64: 1187–1192.
- Koelman DLH, Chahin S, Mar SS, et al. Acute disseminated encephalomyelitis in 228 patients. Neurology. 2016; 86: 2085– 2093.
- Marchioni E, Ravaglia S, Montomoli C, et al. Postinfectious neurologic syndromes: A prospective cohort study. Neurology. 2013; 80: 882–889.
- Chvojka M, Gut J, Jiránek M. Acute disseminated encephalomyelitis. Pediatrie pro Praxi. 2020; 21: 369–373.
- Kirvan CA, Swedo SE, Snider LA, Cunningham MW. Antibodymediated neuronal cell signaling in behavior and movement disorders. J Neuroimmunol. 2006; 179: 173–179.
- Dale RC. Post-streptococcal autoimmune disorders of the central nervous system. Dev Med Child Neurol. 2005; 47: 785–791.
- Chastain EML, Miller SD. Molecular mimicry as an inducing trigger for CNS autoimmune demyelinating disease. Immunol Rev. 2012; 245: 227–238.