
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
An atypical management of subcapsular hydatid cyst: A case report and literature review
Sara Tabassum1; Harsh Bhatia2; FNU Arti3; Maria George4; Zeel Rakeshkumar Patel5; Arlette Villalobos6*
1Dr. V.R.K Women’s Medical College, India.
2Surat Municipal Institute of Medical Education and Research, India.
3Jinnah Sindh Medical University, Pakistan.
4Tbilisi State Medical University, Tbilisi, Georgia.
5GMERS Medical College, India.
5Cardiology/Critical Care Nursing, Ponce Health Sciences University, Puerto Rico.
*Corresponding Author : Arlette Villalobosa
Cardiology/Critical Care Nursing, Ponce Health
Sciences University, Ponce, Puerto Rico.
Email: arlette.villalobos90@gmail.com
Received : Jan 08, 2025
Accepted : Jan 30, 2025
Published : Feb 06, 2025
Archived : www.jcimcr.org
Copyright : © Villalobosa A (2025).
Abstract
Subcapsular hydatid cysts, though relatively rare, present unique management challenges due to their anatomical location and the risk of complications. The PAIR (Puncture, Aspiration, Injection, and Reaspiration) procedure is conventionally contraindicated in subcapsular hydatid cysts due to the risk of rupture and subsequent anaphylaxis. This case report describes a successful PAIR procedure in a patient with a subcapsular hydatid cyst, highlighting the atypical management strategy and its outcomes.
Keywords: Subcapsular hydatid cyst; PAIR procedure; Atypical management; Echinococcosis; Cystic echinococcosis.
Citation: Tabassum S, Bhatia H, Arti F, George M, Villalobos A, et al. An atypical management of subcapsular hydatid cyst: A case report and literature review. J Clin Images Med Case Rep. 2025; 6(2): 3456.
Introduction
Hydatid disease is a potentially serious condition resulting from the ingestion of eggs from the tapeworm Echinococcus granulosus (E. granulosus). The lifecycle of this parasite begins when adult E. granulosus infects canines, primarily dogs, which subsequently shed tapeworm eggs in their feces. Humans become infected through hand-to-mouth transfer of these eggs, leading to the development of hydatid cysts in various organs, predominantly in the liver and lungs [1]. A subcapsular hydatid cyst is specifically located just beneath the liver’s outer surface. This type of cyst poses a significant risk, as its rupture or leakage can lead to serious complications, including infection and anaphylaxis. Management of subcapsular hydatid cysts involves several diagnostic modalities, including blood tests for antibodies against Echinococcus, imaging studies such as CT or MRI for detailed assessment of cyst size and location, and ultrasound for characterizing cyst structure [2].
The initial medical management typically involves the anti-parasitic agent albendazole, which is administered for several weeks preoperatively to shrink the cyst and minimize the risk of spillage during surgical intervention. Surgical management may involve conventional techniques or minimally invasive approaches, such as the Puncture, Aspiration, Injection, Re-Aspiration (PAIR) technique. Conventional surgical methods include total cystectomy, which is the preferred approach for completely removing unruptured cysts. In cases where total cystectomy is not feasible due to factors such as cyst size, location, or proximity to surrounding structures, a partial cystectomy with careful drainage is performed to prevent cyst content spillage. Laparoscopic surgery is an option for smaller cysts when performed by an experienced surgeon [2].
The PAIR technique is a minimally invasive percutaneous treatment used selectively for small, uncomplicated cysts. This procedure involves the ultrasound or CT-guided insertion of a needle into the cyst, followed by aspiration of the cyst fluid. A scolicidal agent, such as hypertonic saline or ethanol, is then injected to eradicate the larvae. After allowing the agent sufficient time to act, the cyst is re-aspirated to remove any remaining fluid. This method is often used in conjunction with alben- dazole to prevent recurrence. However, PAIR is contraindicated in several situations, including proximity to major blood vessels, active biliary communication, large or infected cysts, multilocular cysts, or heavily calcified cysts. Additional caution is warranted for patients who are pregnant or have underlying health conditions that may preclude the procedure, in which case alternative treatments such as surgery or albendazole therapy are recommended [3].
Case presentation
A 45-year-old female presented with a 3-month history of intermittent abdominal pain and discomfort, primarily localized to the right upper quadrant. Her medical history is unremarkable, with no significant past medical issues or known allergies. Upon physical examination, mild tenderness was noted in the right upper quadrant; however, the patient did not exhibit signs of acute distress or rebound tenderness, suggesting a non- emergent condition.
Diagnostic assessment
Ultrasound: Revealed a subcapsular hydatid cyst in the right liver lobe, approximately 7 cm in diameter. The cyst appeared to be near the liver capsule, raising concerns about the risk of rupture.
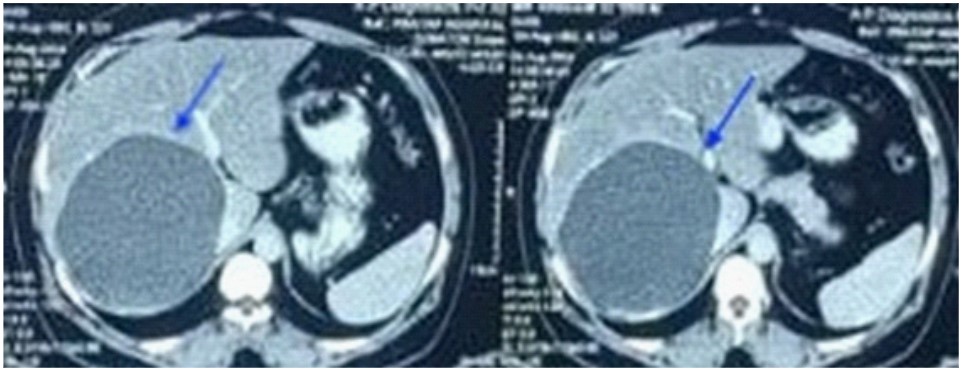
CT scan: Confirmed the presence of a subcapsular hydatid cyst with no signs of cyst rupture or secondary infection. The liver is mildly enlarged, measuring 17 cm in the cranio-caudal direction. The parenchymal texture is homogeneous. A large cystic mass is seen in segments V and VI of the liver, measuring approximately 124×113×129 mm (Figure 1). The lesion shows peripheral calcifications but no perifocal reaction. The interface between the liver and the suprarenal gland is normal. The portal venous system is normal in calibre, and intra-hepatic biliary radicles are not dilated. The porta hepatis is free of lymph nodes.

USG-guided catheter drainage of a right lobe hydatid cyst. The procedure involved insertion of an 18G LP needle into the cyst, with subsequent placement of an 18 Fr. Malecot catheter for drainage as shown in Figure 2. The cyst contents were aspirated, and contrast was injected to rule out communication with biliary channels. Absolute alcohol was used as a scolicidal agent to sterilize the cavity, followed by reaspiration after 20 minutes. Sand samples taken pre- and post-procedure showed no motility, indicating successful treatment. The procedure was performed under aseptic conditions and was uneventful.
Management strategy
Despite the conventional contraindication for PAIR in subcapsular cysts, a multidisciplinary team, including an experienced interventional radiologist and a hepatobiliary surgeon, decided to proceed with the PAIR procedure under controlled conditions. The rationale was based on the cyst’s stability and the patient’s clinical condition, which suggested that a conservative approach might be feasible.
Procedure details
Preparation: The patient was premedicated with antihistamines and corticosteroids to minimize the risk of anaphylactic reaction.
Technique: Under ultrasound guidance, a percutaneous approach was used to puncture the cyst. Aspiration was performed, followed by the injection of hypertonic saline and a scolicidal agent (3% saline solution). The cyst was then reaspirated.
Monitoring: The patient was closely monitored for signs of cyst rupture or anaphylactic reaction during and after the procedure.
Outcome
The PAIR procedure was completed without immediate complications. The patient experienced mild abdominal discomfort, which resolved within 48 hours. Follow-up imaging (ultrasound and CT) at 3- and 6-months post-procedure showed significant reduction in cyst size with no evidence of residual disease or complications.
Discussion
The life-threatening parasitic zoonosis known as hydatid disease with estimated that 2-3 million cases of the disease exist globally. is most prevalent in endemic regions of the Mediterranean Basin, Eastern Europe, North Africa, the Middle East, South America, Australia, and New Zealand where incidence rates are as high as 50 per 100,000 person-years with an estimated prevalence of 10% of the population in highly endemic areas [2]. It is caused by the larvae of Echinococcus granulosus and Echinococcus multilocularis. The disease is spread through the faecal-oral pathway, usually by intimate contact between dogs, sheep, and humans. Dogs act as intermediate hosts in this process of transmission. Approximately 75% of hydatid disease cases involve the liver, with the right hepatic lobe being affected in about 80% of these cases, while the left hepatic lobe accounts for the remaining 20% [4]. The lungs are listed second with 15% of cases, and other organs like the kidneys, spleen, peritoneal cavity, skin, and muscles generally not as frequently affected [5,6].
Hydatid cysts have three distinct layers: [1] the outer Pericyst, composed of host-derived cells like fibroblasts and eosinophils, providing a protective fibrous barrier; [2] the middle laminated acellular membrane, which facilitates nutrient exchange; and [3] the inner germinal layer. Together, the middle and inner layers form the Endocyst, which is notably thicker in the liver. The Pericyst can also be called the Ectocyst. The cyst’s infectious tapeworm larvae, or Scolices, originate from the germinal layer [7]. The WHO-IWGE classification divided hydatid cysts based on their sonographic appearance, activity and viability aiding in the management of Echinococcus granulosus infections.
1. Active cysts include CE1 and CE2. CE1 is an early stage, unilocular, fluid filled, viable cyst. It presents with anechoic with floating protoscolices under ultrasound. On the other hand, CE2 is multivesicular containing multiple daughter cysts, with “Racemose” or “honeycomb” appearance under ultrasound. Both are treated with Antiparasitic therapy, but in case of CE2 cysts surgical intervention is also required due to risk of recurrence and complexity [7].
2. Two kinds of transitional cysts include CE3a, in which the detached germinal layer presents as a “water-lily sign” on ultrasonography, and CE3b, that features partly degenerated daughter vesicles. The course of treatment for the cyst could differ, ranging from PAIR to surgery [7].
3. Inactive cysts include CE4, which exhibits degeneration and solidification, and CE5, which has a thick wall of calcification. Since these stages are normally non-viable and do not need intervention unless difficulties emerge, they are regularly observed [7].
Although hydatid cysts are usually benign being incidental clinical or radiological findings on a routine abdominal ultrasound or an ultrasound performed for diagnosing other pathologies, having them can have serious implications, especially if they are present in important organs like the liver [8]. Anaphylaxis, subsequent infection, and rupture are among the problems that can be effectively avoided with early diagnosis and appropriate medical care. The main complications of hepatic hydatid cysts are rupture and subsequent bacterial infection. In 20-50% of instances, rupture occurs more frequently than secondary bacterial infection, which manifests in 5-8% of cases due to the avascularity of the pericyst and the lack of connection between the endocyst and the host vascular system. Compression of adjacent structures brought on by inflammation or cyst rupture into the peritoneal cavity, pleural space, or bile duct frequently results in symptoms [2,8]. In the study conducted by [5] the symptomatic symptoms might appear in the form of palpable mass in right upper quadrant in abdomen, abdominal pain, loss of appetite, weight loss, and jaundice. In this case the female, 45-year-old patient presented with a 3-month history of intermittent abdominal pain localized to the right upper quadrant with a mild tenderness in the right upper quadrant and negative signs of acute distress or rebound tenderness.
Hydatid cyst diagnosis is based on contemporary imaging techniques, notably Computed Tomography (CT), Magnetic Resonance Imaging (MRI) and ultrasound [7]. Given its accessibility, minimal radiation, and high-resolution ability for assessing cyst characteristics, staging, and directing therapies, ultrasound is the ideal diagnostic method [8]. When ultrasound results are insufficient, CT is preferred with a sensitivity rate of 94% to approach for liver hydatid, especially in obese patients and when calcification, chest, or brain involvement is suspected. Because of their inconsistent sensitivity and specificity, serological tests—such as ELISA utilizing the synthetic peptide p176—are usually reserved for confirmation even though they can validate the diagnosis. Although beneficial, Endoscopic Retrograde Cholangiopancreatography (ERCP) is not always available and is mostly used for therapeutic purposes [7]. In this particular case Ultrasound revealed a 7cm in diameter subcapsular hydatid cyst in right liver lobe and CT scan confirmed that there was no rupture in the cyst or a secondary infection. The cystic mass measuring approximately 124×113×129 mm was present in segments V and VI of the liver with peripheral calcification. The liver was enlarged by about 17 cm in cranial-caudal direction with homogenous appearance, with the portal venous system, intra-hepatic biliary radicles, and interaction with the suprarenal gland all in normal condition and no visible lymph nodes in the hepatic porta.
The treatment approach mainly depends on patient’s symptoms, the radiological stage, the size and location of the cyst(s), the presence of complications and the treating clinicians’ expertise [2]. Currently therapy for Liver Hydatid cysts is multimodal including medical therapy, surgical interventions (conventional or laparoscopic) including conservative and radical approaches in it, a wait and watch approach and in the last two decades minimal invasive percutaneous techniques like percutaneous aspiration, injection and Reaspiration PAIR or PAIR with drainage, PAIR-D has been developed [9,10].
Benzimidazole derivatives, such as Albendazole (ALB) and Mebendazole (MBZ), serve as the mainstay of therapeutic therapy for hepatic hydatid cysts [11]. This is particularly true for smaller, less difficult cysts (<5 cm). When managing individuals who are not candidates for surgery and have many cysts or multiorgan involvement, these anthelmintic drugs can be administered as monotherapy for early-stage cysts (CE1, CE3a) [2,12]. Randomized Controlled Trials (RCTs) have demonstrated that albendazole is more effective than mebendazole, with superior outcomes in terms of cyst degradation and cure rates [11]. Medical management alone is not sufficient to eliminate the cyst entirely. Merely administering medical therapy results in a cure rate of less than 60%, as only approximately 30% of cysts fully resolve [7,12]. For improved outcomes, albendazole is frequently administered as a neoadjuvant before percutaneous or surgical intervention to sterilize the cyst, relieve stress, and lessen the chance of rupture [2,9]. A combination of albendazole treatment for three months and surgical or percutaneous intervention significantly improves cure rates, often exceeding 90% [11,13].
Surgical treatment is considered as the traditional approach towards liver hydatid disease because It guarantees total removal of the parasite, is safe and efficient with mortality rate of only 0.9-3.6%, requires no intraoperative shedding, protects healthy tissues, and lowers the risk of long-term recurrence of around 11.3% in the first 5 years and cavity-related difficulties [9,14]. Surgery is indicated for bigger liver cysts (>10 cm), and cysts at risk of rupture and/or complicated cysts [12]. Based on how the pericyst is approached, classical surgical techniques for hepatic hydatid cysts are divided into different categories. These include cystectomies (procedures without pericyst resection) and resection-related ones (hepatectomy, partial pericystectomy, and pericystoresection). Options for managing the residual cavity include pericystobiliary drainage, anastomosis with the stomach/jejunum for drainage, padding, omental plombage, bipolar drainage of the cavity and bile duct, and external drainage [9]. The radical approach, also known as a total cystectomy or pericystectomy, entails the complete removal of the cyst, including the pericyst, along with the damaged tissue. In contrast, the conservative approach, also known as a partial cystectomy, comprises the partial removal or draining of the cyst while maintaining the surrounding tissue. Radical approach is a more aggressive surgical technique that lowers the chance of recurrence by resectioning the affected organs or performing a hepatectomy [11]. When major surgery poses a risk, such as when a cyst is placed in a difficult-to-reach area or in a patient with numerous conditions, conservative treatment is carried out [2]. Open surgery is considered highly controversial since it can cause anaphylactic shock, death, and intraperitoneal spillage while performing puncture. Study conducted by Bayrak et al. suggested that laparoscopic surgeries are much more safer with small incisions, less postoperative pain, decreased risks of wound infections, faster healing, less blood loss, and shorter hospital stays and operation times and a recurrence rate of 2.7% in laparoscopic procedure to 4.7% in open surgery [15,16]. But laparoscopic approach is scarcely widespread, expensive, requiring special devices and experience, being suitable for selected cases like where cysts are located superficially on the anterior surface of the liver without communicating with the biliary tree [9].
Alternative approach other than chemotherapy and surgery are the percutaneous techniques which are considered minimally invasive procedures. These include PAIR, PAIRD, Modified Catheterisation Technique (MoCaT) or Percutaneous Evacuation (PEVAC) with a known superiority of PAIR over catheterisation [17]. In the PAIR procedure, Cysts are initially identified using ultrasound guidance in order to carry out this surgery. After that, a local anaesthetic is used to puncture the cyst percutaneously. Following the aspiration of cystic fluid, scolicidal chemicals such as alcohol, betadine or cetrimide, hypertonic saline, and others are injected into the cyst cavity. Ultimately, the injected solution is re-aspirated after 20 to 30 minutes [16]. PAIR-D is a variation of PAIR where intracystic catheter is inserted at the conclusion of the procedure and after 24hours the cavity is emptied and irrigated with saline solution [9]. PAIR has established itself as a reliable, commercially efficient, high success rate procedure especially for CE1 and CE3a cysts and for CE2 cyst which is debatable [9,16,17]. It is indicated in patients who are contraindicat- ed for surgery, suffer post-surgical relapses, refuse surgery, or have multiple accessible cysts, in addition to hydatid cysts with daughter vesicles, detached membranes, and superinfected cysts. It is also utilized in pregnant women and people who do not react to medication therapy. Patients who are uncooperative, inactive or calcified cysts, cysts that cannot be punctured, and cysts that communicate with the biliary tree are among the contraindications. Serologic and imaging tests must be used in conjunction with careful monitoring due to the possibility of subsequent hydatidosis. For surgical relapses, inoperable cases, or albendazole therapy as the first line of treatment for CE1 and CE3a cysts, PAIR is advised. Many studies have concluded that PAIR with albendazole as prophylaxis is better than surgery and the first choice for uncomplicated HCs [11,18,19]. This is further proven right, despite concerns over the subcapsular location, the PAIR procedure was performed successfully. Critical elements contributing to its success included the use of premedication to prevent anaphylaxis, careful ultrasound-guided puncture, and the use of a scolicidal agent to sterilize the cyst cavity. The lack of biliary communication, as confirmed by contrast injection, further ensured a safe outcome. The patient’s post-procedural course, including significant cyst size reduction and absence of complications at follow-up, supports the efficacy and safety of PAIR in this unconventional case
The PAIR procedure is a valuable tool in the management of hydatid cysts; however, its use in subcapsular cysts is fraught with risk due to potential rupture and serious allergic reactions. This case illustrates that, with careful patient selection, proper premedication, and stringent monitoring, PAIR can be successfully performed even in subcapsular hydatid cysts. The favourable outcome in this patient suggests that, while traditionally contraindicated, PAIR may be considered in specific scenarios with appropriate safeguards.
Conclusion
This case report demonstrates that, contrary to conventional recommendations, the PAIR procedure can be successfully and safely employed in the management of subcapsular hydatid cysts under controlled conditions. Further studies and reports are needed to refine the indications and protocols for using PAIR in such challenging cases.
Declarations
Acknowledgments: We thank the interventional radiology and hepatobiliary surgery teams for their expertise and support in this case.
Conflicts of interest: The authors declare no conflicts of interest.
Funding: No funding was received for this case report.
References
- Hydatid disease. Communicable disease control guidance. 2024. Available from: https://www.health.qld.gov.au/disease-control/ conditions/hydatid-disease
- Govindasamy A, Bhattarai PR, John J. Liver cystic echinococcosis: a parasitic review. Ther Adv Infect Dis. 2023; 10: 20499361231171478.
- Regmee S, Maharjan DK, Thapa PB. The Current Protocols in the Management of Hepatic Hydatid Disease. Indian J Surg. 2021; 83: 810–7.
- Ahire P, Iyer N, Gada PB. Complication of Hepatic Hydatid Cyst Surgery Presenting as Obstructive Jaundice. Cureus. 2023; 15: e35410.
- Baruah A, Sarma K, Barman B, Phukan P, Nath C, Boruah P, et al. Clinical and Laboratory Presentation of Hydatid Disease: A Study from Northeast India. Cureus. 2020; 12: e10260.
- Nayman A, Guler I, Keskin S, Erdem TB, Borazan H, Kucukapan A, et al. A novel modified PAIR technique using a trocar catheter for percutaneous treatment of liver hydatid cysts: a six-year experience. Diagn Interv Radiol. 2016; 22: 47–51.
- Alshoabi SA, Alkalady AH, Almas KM, Magram AO, Algaberi AK, Alareqi AA, et al. Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker. Diagnostics. 2023; 13: 1127.
- Alexiou K, Mitsos S, Fotopoulos A, Karanikas I, Tavernaraki K, Konstantinidis F, et al. Complications of Hydatid Cysts of the Liver: Spiral Computed Tomography Findings. Gastroenterol Res. 2012; 5: 139–43.
- Botezatu C, Mastalier B, Patrascu T. Hepatic hydatid cyst – diagnose and treatment algorithm. J Med Life. 2018; 11: 203–9.
- Gupta N, Javed A, Puri S, Jain S, Singh S, Agarwal AK. Hepatic hydatid: PAIR, drain or resect? J Gastrointest Surg Off J Soc Surg Aliment Tract. 2011; 15: 1829–36.
- Gomez i Gavara C, López-Andújar R, Belda Ibáñez T, Ramia Ángel JM, Moya Herraiz Á, Orbis Castellanos F, et al. Review of the treatment of liver hydatid cysts. World J Gastroenterol WJG. 2015; 21: 124–31.
- Ferrer Inaebnit E, Molina Romero FX, Segura Sampedro JJ, González Argenté X, Morón Canis JM. A review of the diagnosis and management of liver hydatid cyst. Rev Esp Enferm Dig. 2022; 114: 35–41.
- Velasco-Tirado V, Alonso-Sardón M, Lopez-Bernus A, Romero-Alegría Á, Burguillo FJ, Muro A, et al. Medical treatment of cystic echinococcosis: systematic review and meta-analysis. BMC Infect Dis. 2018; 18: 306.
- Daduk Y, Seker A, Sozutek A, Olmez T, Kaplan K, Dur H, et al. Treatment Options and the Management of Complications in Hydatid Cysts of the Liver in Endemic Regions. Ann Ital Chir. 2024; 95: 213–9.
- Bayrak M, Altıntas Y. Current approaches in the surgical treatment of liver hydatid disease: single center experience. BMC Surg. 2019; 19: 95.
- Sokouti M, Sadeghi R, Pashazadeh S, Abadi SEH, Sokouti M, Ghojazadeh M, et al. A systematic review and meta-analysis on the treatment of liver hydatid cyst using meta-MUMS tool: comparing PAIR and laparoscopic procedures. 2020.
- Akhan O. Percutaneous treatment of liver hydatid cysts: to PAIR or not to PAIR. Curr Opin Infect Dis. 2023; 36: 308–17.
- Crippa FG, Bruno R, Brunetti E, Filice C. Echinococcal liver cysts: treatment with echo-guided percutaneous puncture PAIR for echinococcal liver cysts. Ital J Gastroenterol Hepatol. 1999; 31: 884–92.
- Peláez V, Kugler C, del Carpio M, Correa D, López E, Larrieu E, et al. Treatment of hepatic hydatid cysts by percutaneous aspiration and hypertonic saline injection: results of a cooperative work. Bol Chil Parasitol. 1999; 54: 63–9.