
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Infectious mononucleosis with hoagland sign
*Corresponding Author : Ranveer Singh Jadon
Additional Professor, Department of Medicine, All
India Institute of Medical Sciences, Medicine Office,
3rd floor, Teaching Block, AIIMS, New Delhi 110029,
India.
Tel: +91-9540951048;
Email: dr.ranveerjadon@yahoo.co.in
Received : Jan 08, 2025
Accepted : Jan 30, 2025
Published : Feb 06, 2025
Archived : www.jcimcr.org
Copyright : © Jadon RS (2025).
Abstract
This case report describes the clinical challenges encountered in a 15-year-old girl presenting with forehead and periorbital swelling, fever, cough, and respiratory distress. Initial diagnosis of orbital cellulitis yielded limited response to antibiotics. Subsequent investigations revealed pancytopenia, elevated ferritin, creatinine kinase, and lactate dehydrogenase, as well as bilateral pleural effusion. Despite considering disseminated tuberculosis, malignancy, and connective tissue disorder, the exact etiology remained elusive. Autoimmune markers and myositis panels were unyielding. The provisional diagnosis of Ebstein Barr Virus (EBV) infection was established based on clinical indicators, supported by positive EBV viral capsid antigen. Spontaneous resolution of symptoms and inflammatory markers, alongside improved neutrophil levels, led to the patient’s discharge. Subsequent follow-up highlighted a gradual reduction in eyelid swelling.
Keywords: Ebstein barr virus; Periorbital swelling; Infectious mononucleosis; Hemophagocytosis.
Citation: Sikdar S, Priyadarshi M, Mandal S, Sinha S, Jadon RS. Infectious mononucleosis with hoagland sign. J Clin Images Med Case Rep. 2025; 6(2): 3457.
Introduction
A 15-year-old female patient with no previous medical conditions presented to the emergency department with several complaints over the past two months. She was experiencing swelling of her forehead and area around the eyes, intermittent low-grade fever, dry cough with a sore throat, and shortness of breath that worsened over the past 15 days. The swelling initially started on the forehead and progressed to the eyelids with redness. Eventually, the patient was unable to open her eyes due to the swelling.
An MRI of the orbits revealed subcutaneous edema in the pre-maxilla and forehead, affecting both upper and lower eyelids. The initial diagnosis was orbital cellulitis, and the patient was started on antibiotics. However, there was little to no response.
Further evaluation showed pancytopenia, elevated levels of ferritin, creatinine kinase, and Lactate Dehydrogenase (LDH), and bilateral pleural effusion. Considering these, diagnosis of disseminated tuberculosis, malignancy or a connective tissue disorder were kept.
Pleural fluid analysis indicated an exudative picture with a predominance of lymphocytes and an ADA (Adenosine Deaminase) level of 82 U/L with molecular tubercular genetic tests were negative. Autoimmune markers, such as anti-nuclear anti-bodies, anti-neutrophilic cytoplasmic antibodies, extra-nuclear antibody profile, and rheumatoid factor, were also negative. A bone marrow examination was performed, which showed hemophagocytosis and functional bone marrow. A skin biopsy was conducted to investigate the possibility of Connective Tissue Disease (CTD), but it showed nonspecific inflammatory changes.
The patient exhibited proximal muscle weakness, and a whole-body PET-CT scan revealed uptake in multiple muscles, including those in the face, frontal region, accessory muscles of respiration, bilateral proximal muscles of the upper limbs, and parts of the gluteus muscle and pelvic diaphragm, indicative of polymyositis. However, the myositis panel came back negative.
A provisional diagnosis of Ebstein Barr virus infection was made based on the patient’s history of sore throat, resolving pancytopenia, exudative lymphocytic pleural effusion, and swollen eyelids. The serum EBV PCR results were negative, but the EBV viral capsid antigen was positive.
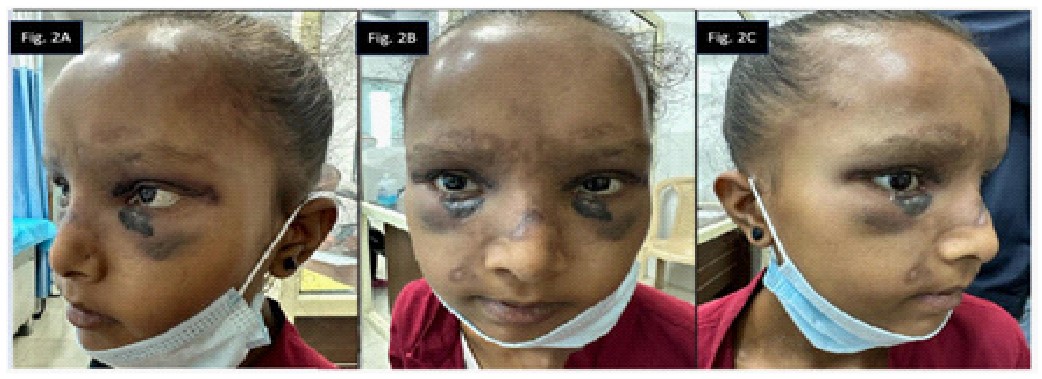
Over time, the patient’s inflammatory markers decreased spontaneously, and neutrophil levels showed improvement. When the patient’s condition stabilized, she was discharged. Two months later, during a follow-up in the outpatient department, it was observed that the eyelid swelling had gradually reduced (Figures 2A & 2B).
Discussion
Epstein-Barr Virus (EBV) is a ubiquitous pathogen that may cause a wide range of systemic diseases. Infectious Mononucleosis (IM), often known as glandular fever, is one of them [1]. Bilateral periorbital oedema, sometimes known as the ‘Hoagland sign,’ is a less common clinical symptom [2]. The Hoagland sign, which appears at the start of the disease or throughout its progression, only lasts a few days to a few weeks [3]. IM is a self-limiting systemic infection presenting as fever, pharyngitis, and cervical chain lymphadenopathy. In some cases, myositis and even pleural effusion has also been noted. Rarely the disease can also progress to have Hemophagocytic Lymphohistiocytosis (HLH) [1].
Bilateral periorbital oedema (Hoagland sign) may also be present and can precede or appear early in the illness course. It was originally recognised in the 1950s, when it was discovered in up to one-third of IM cases [4]. However, the incidence of this disease is much poorer in clinical practice.
The pathogenesis of ocular involvement in IM is not fully understood. Based on the finding that reactive cervical lymphadenopathy usually leads in glandular oedema, HM Bass hypoth- esised that impeded lymphatic drainage may explain oedema, with the proviso that the latter is linked with inflammation whereas the former is not [5]. Magnetic resonance imaging revealed localised subcutaneous oedema in a case described by Süer et al as it was so in our case as well [6]. On the contrary, Burger et al. and Aburn et al. revealed radiographic evidence of lacrimal gland inflammation (dacryoadenitis), which supports the virus’s alleged gravitation towards lymphoid organs, culminating in leukocyte proliferation [7,8].
If present, the Hoagland sign is generally self-resolving. Without therapy, oedema resolves after a few days. Some case reports reported somewhat lengthier intervals of up to two weeks before complete resolution [9]. When airway patency is compromised, the majority of treatment is systemic corticosteroid, which has also been demonstrated to result in fast oedema dampening, albeit its efficacy remains subjective.
Periorbital cellulitis, angioedema, Cytomegalovirus (CMV) infection, and nephrotic and nephritic syndromes are all possible causes of bilateral periorbital oedema. Pre-septal cellulitis and angioedema were improbable due to the absence of other cardinal symptoms of inflammation (pain, erythema, and warmth) and a lack of atopic characteristics. While CMV infection can cause symptoms similar to mononucleosis.
Learning point for clinicians
1. Infectious mononucleosis can present with bilateral upper eyelid swelling called the Hoagland sign.
2. EBV has a myriad of presentations and high clinical suspicion is necessary to come to a diagnosis.
3. Clinically diagnosing Hoagland sign alleviates the patient from undergoing unnecessary investigations.

Declarations
Acknowledgements: We thank all the personnel of our out-patient clinic, including nurses, doctors and residents. No funding was received for this research paper.
Ethical approval: A written informed consent was obtained from the patient. (It has been attached with the supplementary material). This is a case report and no approval from the AIIMS research ethics committee was required.
Financial support: No funding was received to assist with the preparation of manuscript. The authors have no financial and non-financial interests to disclose.
Disclosure: There are no competing interests related to the authors of this manuscript.
References
- Naughton P, Healy M, Enright F, Lucey B. Infectious Mononucleosis: diagnosis and clinical interpretation. Br J Biomed Sci. 2021; 78:107–16.
- Bronz G, Zanetti BPESM, Bianchetti MG, Milani GP, Lava SAG, Neuhaus TJ, et al. Bilateral upper eyelid swelling (Hoagland sign) in Epstein-Barr infectious mononucleosis: prospective experience. Infection. 2023; 51: 471–4.
- Otsuka Y, Kishida M. Hoagland sign: bilateral upper eyelid oedema. BMJ Case Rep. 2022; 15: e250857.
- Hoagland RJ. Infectious mononucleosis. Am J Med. 1952; 13(2): 158-71.
- Bass MH. Periorbital edema as the initial sign of infectious mononucleosis. J Pediatr. 1954; 45: 204–5.
- Suer KH, Kaptanoglu AF. Association of Periorbital Edema and Fever in Acute Infectious Mononucleosis: A Case Report. Kafkas J Med Sci. 2013; 3: 152–4.
- Burger J, Thurau S, Haritoglou C. Beidseitige Oberlidschwellung bei Mononucleosis Infectiosa (Hoagland-Zeichen). Klin Monbl Augenheilkd. 2005; 222: 1014–6.
- Aburn NS, Sullivan TJ. Infectious Mononucleosis Presenting with Dacryoadenitis. Ophthalmology. 1996; 103: 776–8.
- van Hasselt W, Schreuder RM, Houwerzijl EJ. Periorbital oedema. 67(8): 338.