
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 6
Splenic injury following trivial trauma presenting as shoulder pain: A case report
*Corresponding Author : Vaishnavi Thevrekandy
Department of Gastroenterology, Postgraduate
Institute of Medical Education and Research,
Chandigarh, India.
Email: vaishnavisajeev6@gmail.com
Received : Jan 11, 2025
Accepted : Feb 03, 2025
Published : Feb 10, 2025
Archived : www.jcimcr.org
Copyright : © Thevrekandy V (2025).
Citation: Thevrekandy V. Splenic injury following trivial trauma presenting as shoulder pain: A case report. J Clin Images Med Case Rep. 2025; 6(2): 3460.
Introduction
The spleen is the most commonly injured visceral organ in blunt abdominal trauma, primarily due to motor vehicle crashes, with direct abdominal blows and falls being significant contributing factors to traumatic rupture [1]. Additionally, traumatic rupture can present immediately after an injury or may present in a delayed fashion [1]. The lack of substantial trauma does not exclude the possibility of splenic injury [2]. Following trauma to spleen patients may present with hypovolemic shock manifesting as tachycardia, hypotension, and other findings include tenderness to palpation in the left upper quadrant, generalized peritonitis, or referred pain to the left shoulder (Kehr sign) [3]. Delayed splenic rupture is a rare case following major traumatic events and even rarer following trivial trauma [4]. Here we present 2 cases of hemodynamically stable splenic injury following trivial trauma presented with left shoulder pain. Case 1 presented after 4 days of trivial trauma to abdomen.
Case presentations
Case 1
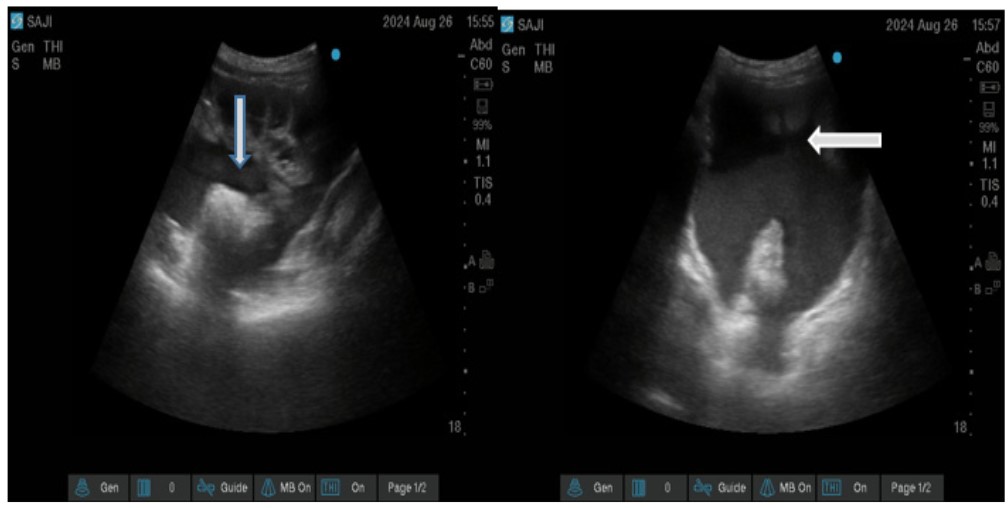
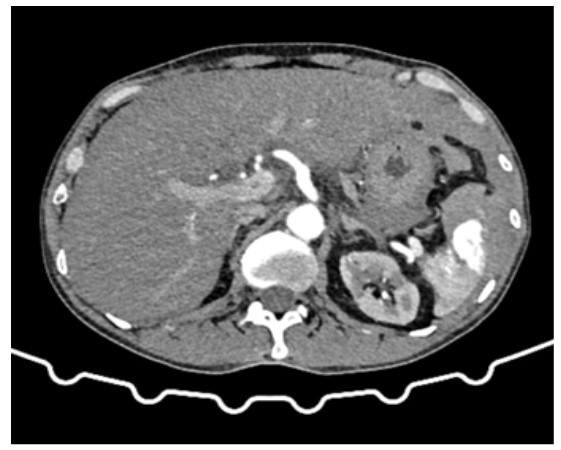
55-year-old male patient shop keeper by occupation, presented to ED with complaints of left shoulder pain for 1 day. He was initially treated in a local hospital near his home for the same complaints. But there was no symptomatic improvement in pain hence he was referred to our hospital. He did not disclose any chest pain, diaphoresis, difficulty in breathing, fever, or pain abdomen. On examination his cardiorespiratory parameters were within normal limits (Non-invasive blood pressure of 118/78 mmhg, pulse rate of 82 beats per minute, respiratory rate of 16 per minute, peripheral oxygen saturation of 98% on room air). On local examination there was no visible contusions or tenderness over the left shoulder, range of motion was full but painful. The abdominal examination showed minimal tenderness in the left hypochondrium with normal bowel sounds. Other systemic examination was unremarkable. He reported an initial Pain score of 6/10 at the left shoulder joint by numerical rating scale and iv analgesics was given. Further history revealed that the patient had an accidental slip and fall onto a hard surface while working in his shop with impact on his abdomen 4 days back. Extended Focused Assessment with Sonography for Trauma (E-FAST) scan showed fluid collection in the suprapubic view (Figure 1). Electrocardiogram was normal. In view of positive E-FAST, a contrast enhanced computed tomography scan of abdomen was performed and confirmed that the patient had a Grade V splenic injury with moderate hemoperitoneum (Figure 2). He was then taken to operating room for emergency splenectomy.
Case 2
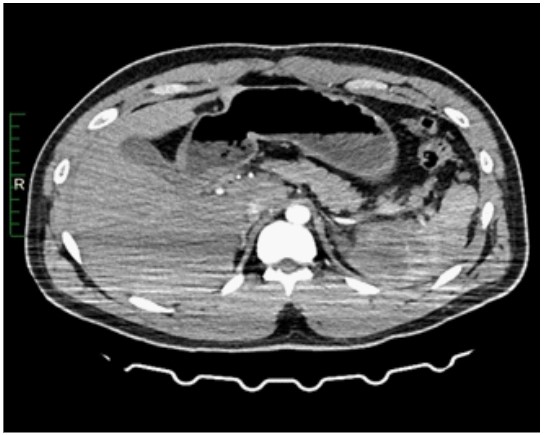
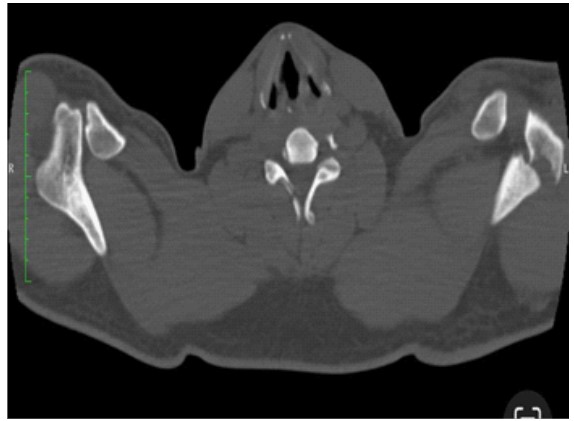
28-year-old male presented to emergency department with complaints of pain over left shoulder joint following skid and fall from a bicycle 5 hours back. On initial evaluation his vital were within normal limits (respiratory rate of 18 per minute, peripheral oxygen saturation of 100% on room air, Non-invasive blood pressure of 126/81 mmhg, pulse rate of 78 beats per minute). On local examination he had an abrasion over left shoulder joint with mild swelling and tenderness on palpation. His initial pain score was 7/10 which we have managed with iv analgesics On Extended Focused Assessment with Sonography for Trauma (E-FAST) scan showed free fluid in Morrison’s pouch. Contrast enhanced computed tomography scan of abdomen confirmed that he had a grade III splenic injury with mild hemoperitoneum (Figure 3). X-ray left shoulder was suspicious of fracture of left acromion process, and confirmed that with a plane CT chest with shoulder joint (Figure 4). Since the patient’s hemodynamics were stable non-operative management was chosen.
Clinical discussion
Among blunt abdominal trauma spleen is the most commonly injured organ. Injury to the spleen may be suspected on the basis of the patient’s mechanism of injury and physical examination findings, but definitive diagnosis generally requires further diagnostic testing. A visual inspection for signs of external trauma such as abrasions, lacerations, contusions, and classic seatbelt sign on the abdomen is beneficial [1]. The lack of external visual findings does not exclude the possibility of intra-abdominal pathology, as up to 20% of patients with such injuries may not exhibit clinically apparent symptoms [1]. Spontaneous splenic rupture or pathologic splenic rupture can occur after negligible trauma or insignificant events [2]. Abdominal CECT is the gold standard to determine the grades of injury in hemodynamically stable patients. An intraparenchymal or subcapsular hematoma is also easier to identify and sometimes associated with delayed splenic rupture [5]. American Association for the Surgery of Trauma (AAST) splenic injury scale, is the most widely used grading system for splenic injury [6]. A positive FAST scan is an absolute indication for emergency exploratory laparotomy for hemodynamically unstable patients. However, a negative FAST scan cannot reliably exclude intraabdominal hemorrhage [7].
Through this case report, we want to emphasize that clinicians should keep an eye on the risk of Delayed Splenic Rupture even after trivial abdominal trauma. Isolated left shoulder pain following a motor vehicle crash may indicate spleen rupture, especially in the absence of visible trauma to the left clavicle or shoulder. This is due to the innervation of the diaphragm which sits above the spleen in the left upper quadrant (Kehr sign) [1]. However, history of minor trauma might have been overlooked in these cases. Hence, a detailed history of major or minor trauma in the preceding weeks must be elicited for any patients presenting with abdominal pain.
Conclusion
Even after trivial trauma, patients can present with splenic injury which can be immediate or delayed. Emergency physician should consider the entire clinical scenario for evaluation of the patient. In any patients presenting with isolated left shoulder pain in the background of minor or major trauma in the preceding weeks, keep a high suspicion on spleen injury.
References
- Akoury T, Whetstone DR. Splenic Rupture. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK525951/
- Reinhold GW, Melonakos TK, Lyman DT. A Near Fatal Sneeze Spontaneous Splenic Rupture: A Case Report and Review of the Literature. Clin Pract Cases Emerg Med. 2017; 1: 190-193.
- Söyüncü S, Bektaş F, Cete Y. Traditional Kehr’s sign: Left shoulder pain related to splenic abscess. Ulus Travma Acil Cerrahi Derg. 2012; 18: 87-8.
- Basukala S, Tamang A, Bhusal U, Sharma S, Karki B. Delayed splenic rupture following trivial trauma: A case report and review of literature. Int J Surg Case Rep. 2021; 88: 106481.
- Gamblin TC, Wall CE Jr, Royer GM, Dalton ML, Ashley DW. Delayed splenic rupture: case reports and review of the literature. J Trauma. 2005; 59: 1231-4.
- Kozar RA, Crandall M, Shanmuganathan K, Zarzaur B, Coburn M, Cribari C, et al. AAST Patient Assessment Committee. Reply to Letter: Organ injury scaling 2018 update: Spleen, liver, and kidney. J Trauma Acute Care Surg. 2019; 87: 999.
- Schnüriger B, Kilz J, Inderbitzin D, Schafer M, Kickuth R, Luginbühl M, et al. The accuracy of FAST in relation to grade of solid organ injuries: a retrospective analysis of 226 trauma patients with liver or splenic lesion. BMC Med Imaging. 2009; 9: 3.