
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A behemoth rhinolith: Case report and review of literature
Zia Zafar, MS, ENT1; Tanuj Madan, MS, ENT1; Vikas Sharma, MCh1*; Samrat Ghosh, MD2; Manoj Gopal Madakshira, DM3; Vaddepally Bala Krishna, MS, ENT1; Dibangkar Das, MS, ENT1; P Praveen Kumar, MS, ENT1; Siddalingesh Hugar, MS, ENT1
1Department of Otolaryngology & Head and Neck Surgery, Command Hospital Kolkata, India.
2Department of Radiology, Command Hospital Kolkata, India.
3Department of Pathology, Command Hospital Kolkata, India.
*Corresponding Author : Vikas Sharma, MCh
Department of Otolaryngology & HNS, Command
Hospital, Kolkata-700027, India.
Tel: +750-036-5337
Email: vicky251983@gmail.com
Received : Jan 14, 2025
Accepted : Feb 04, 2025
Published : Feb 11, 2025
Archived : www.jcimcr.org
Copyright : © Sharma V (2025).
Abstract
Introduction: Rhinolith which translates to stone formation within the nasal cavity is a rare and under-diagnosed condition. The available literature is scanty and tends to be in the form of isolated case reports and very few case series. It is, therefore, important to report each case to facilitate its valid statistical analysis. Its etiopathogenesis is vaguely recognized. They are the result of deposition of nasal, lacrimal and inflammatory mineral salts by accretion around an endogenous or exogenous nidus, usually neglected foreign bodies.
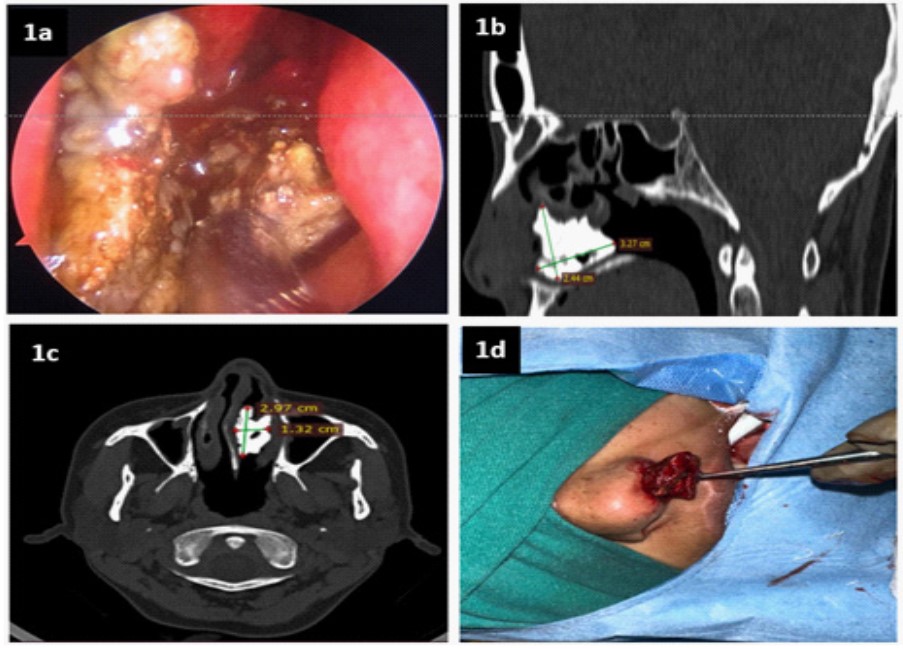
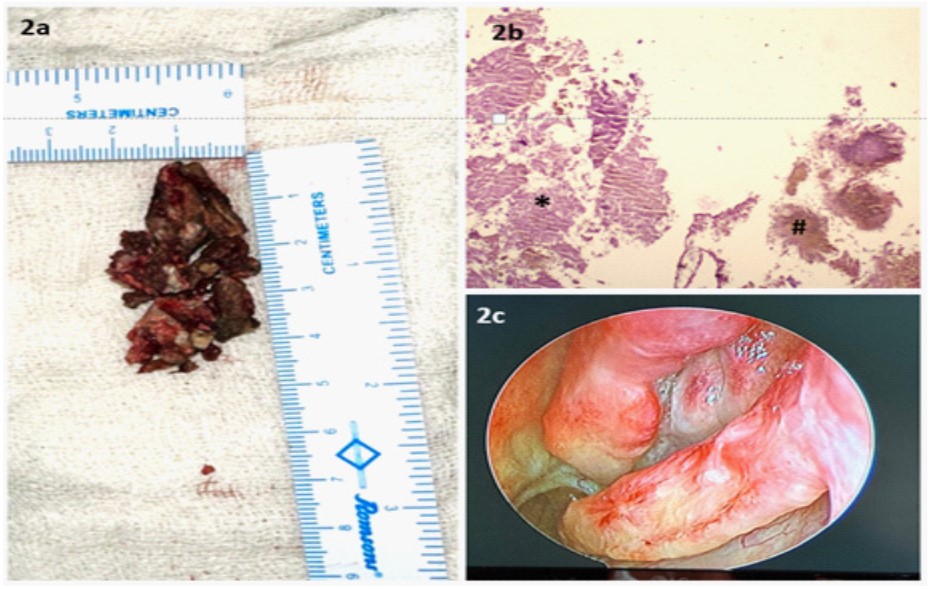
Case report: 33 years old female, reported with complaint of left sided nasal obstruction with history of recurrent epistaxis and foulsmelling mucopurulent discharge from left nasal cavity. Left nasal cavity showed blackish brown, stony hard mass filling the entire nasal cavity. Contrast-enhanced computed tomogram of nose and parasnasal sinuses revealed a well-defined geographical calcific (HU~1789) density in the left nasal cavity between nasal septum and in inferior meatus measuring ~2.1×1.1×2.3 cm. Intra-operatively, the extent of rhinolith was confirmed after decongestion. Rhinolith was freed from all points of contact viz. septum, middle turbinate and inferior turbinate. It was removed piecemeal (Figure 1d). Post-operative period was uneventful. Histopathological Report (HPR) revealed dystrophic calcification with granulation tissue surrounded with adherent actinomyces colonies.
Conclusion: Literature appraisal brings out that despite being sporadic in incidence, its susceptible population includes children and young adults as they insert foreign bodies in nose. We present a case of 35 years old female with a giant rhinolith in left nasal cavity which was removed with endonasal endoscopic approach.
Keywords: Foreign body; Nasal obstruction; Rhinolithiasis; Calcification; Epistaxis; Nasal septum; Foul smelling; Granulations; Coblator; Exogenous.
Citation: Zafar Z, Madan T, Sharma V, Ghosh S, Madakshira MG, et al. A behemoth rhinolith: Case report and review of literature. J Clin Images Med Case Rep. 2025; 6(2): 3463.
Introduction
Rhinoliths (Greek, rhino~ nose and lithos ~ stone) are hard and dense stone like calcifications within nasal cavity formed by build-up of nasal, lacrimal and inflammatory mineral salts by accrual around an endogenous (i.e. ectopic tooth, bone chip, blood clot, mucus, bacteria, necrosed mucosa) or exogenous (i.e. fruits seeds, gauze, pebbles, plant material, cotton wool, plastic, insects, beads, dental imprinting material, remnants of nasal tampons etc.) nidus [1]. Despite foreign body nose being common in Otorhinolaryngology (ORL) clinics, rhinoliths are extremely rare and are seen in 0.01% of these patients [2]. The principal account of Rhinolithiasis is credited to Bartholin in 1654 [5]. The first radiological description came from Maclin-type in 1900 [6]. Owing to its rarity and under-diagnosis till date approximately 700 such cases have been reported [7]. They are calcareous concretions formed from precipitation of mineral salts on intranasal foreign body which may be of endogenous or exogenous origin. These nidi are absent in about 50 percent of cases indicating an organic origin which degrades over time [7].
The incidence quoted in the literature is approximately 1 in 10,000 ORL patients [7]. But, its actual value is probably higher owing to its incidental diagnosis in asymptomatic patients and obscured symptomatology due to co-existent nasal pathologies [7]. They are mostly unilateral and reported in third decade of life, rarely in children and mostly in female patients [8]. Bilateral rhinoliths are extremely rare [9]. In our reported case, the patient is a female but in fourth decade of her life.
They are mostly asymptomatic and are incidentally picked upon panoramic imaging [3]. However, patients may present with unilateral nasal symptoms like obstruction, fetid rhinorrhea, anosmia, epistaxis, taste and smell disturbances, and headache along with signs of sinusitis [4]. A high index of suspicion is required to diagnose a forgotten entity like this.
Case report
33 years old female, a known case of Carcinoma Breast (Right) post modified radical mastectomy (pT2N3M0) post adjuvant chemoradiotherapy (completed 2 years prior to the date of presentation) presently on Tamoxifen, reported with complaint of left sided nasal obstruction of 2 months duration. It was insidious, continuous and gradually progressive. Patient also gave history of recurrent epistaxis and foul-smelling mucopurulent discharge from left nasal cavity. However, spouse gave history of experiencing bad smell in close proximity with her. Patient denied any foreign body insertion in nose or previous nasal surgery. Clinical examination revealed Grade II deviation of nasal septum towards right. Left nasal cavity showed blackish brown, stony hard mass filling the entire nasal cavity extending between the lateral nasal wall and septum; polypoidal middle turbinate (Figure 1a). No growth or mucopus was seen. Rest of ORL examination was essentially normal. With the presumptive diagnosis of Rhinolith/neglected foreign body left nasal cavity, a contrast- enhanced computed tomogram of nose and parasnasal sinuses (CECT nose and PNSs) was done which revealed a well-defined geographical calcific (HU~1789) density in the left nasal cavity between nasal septum and in inferior meatus measuring ~2.1×1.1×2.3 cm with surrounding soft tissue content (Figure 1b). The calcific lesion was abutting and displacing the nasal septum to the right with mild erosion; laterally, it was flush with medial wall of left maxillary sinus; posteriorly extent was just proximal to choana and inferiorly, it was abutting the nasal floor (Figure 1c). Patient was taken up for examination under General Anesthesia (GA). Intra-operatively, the extent of rhinolith was confirmed after decongestion. Rhinolith was freed from all points of contact viz. septum, middle turbinate and inferior turbinate. It was removed piecemeal (Figure 1d). All pieces were oriented as per the intraoperative findings (Figure 1d). Granulation tissue and soft tissues of nasal cavity was removed using coblator. Post-operative period was uneventful. Histopathological Report (HPR) revealed dystrophic calcification with granulation tissue (Figure 2b) surrounded with adherent actinomyces colonies (Figure 2b). Patient has been on regular follow up with check nasal endoscopies which reveal a well mucosalised nasal cavity (Figure 2c).
Discussion
The principal account of Rhinolithiasis is credited to Bartholin in 1654 [5]. The first radiological description came from Maclintype in 1900 [6]. Owing to its rarity and under-diagnosis till date approximately 700 such cases have been reported [7]. They are calcareous concretions formed from precipitation of mineral salts on intranasal foreign body which may be of endogenous or exogenous origin. These nidi are absent in about 50 percent of cases indicating an organic origin which degrades over time [7].
The incidence quoted in the literature is approximately 1 in 10,000 ORL patients [7]. But, its actual value is probably higher owing to its incidental diagnosis in asymptomatic patients and obscured symptomatology due to co-existent nasal pathologies [7]. They are mostly unilateral and reported in third decade of life, rarely in children and mostly in female patients [8]. Bilateral rhinoliths are extremely rare [9]. In our reported case, the patient is a female but in fourth decade of her life.
The pathogenesis of this entity remains cryptic. Nevertheless, various factors have been postulated as its contributors. Entry and impaction of foreign body into the nasal cavity causes obstruction leading to downturn of nasal secretions. This incites local inflammatory response with deposition of salts of calcium, aluminium, magnesium, iron and organic substances like glycine and glutamic acid leading to slow and gradual increase in its size. The route of entry to nose is mostly anterior but, in few cases, a foreign body may get lodged into nasal cavity following posterior path through choana during sneezing, coughing or emesis [9].
Rhinoliths cause non-specific symptoms like chronic unilateral nasal obstruction, maxollo-facial region pain (direct stimulation, referred pain, mucosal contact), purulent rhinorrhea, nasal bleed, epiphora, and taste and smell disturbances [7,8].
They are usually formed in inferior meatus. Clinically, patients may have nasal septal deviation to opposite side, erosion and/ or septal perforation, variable extent of erosion of lateral nasal wall finally culminating into an oro-antral or oro-nasal fistula [7]. Examination with probe reveals irregular, grayish-black to brownish bony hard mass. A nasal polyp may be seen surrounding a rhinolith which is due to long standing mucosal irritation [8].
Co-existent sinusitis has also been reported in about 20 percent cases [7]. Few complicated cases reported also mention intra-cranial extension, middle otitis and dacryocystitis [8].
Its differential diagnoses include calcified sinonasal masses encompassing osteoma, odontoma, calcified polyps, nasal glioma, encondroma, hemangioma, ossifying fibromas, calcifying angiofibromas, septal desmoid tumours, malignant tumours, syphilis and calcified tuberculomas [8]. Radiological and histopathological examination clinches the diagnosis.
An office nasal endoscopy is essential to locate the rhinolith. Computed Tomography (CT)/ Cone beam CT is the investigation of choice. It enables exact localization, measurement of dimensions, visualization of internal features like central radiolucency of organic nidus surrounded by opacity, local tissue reactions and also offers differential diagnosis of other radio-opaque masses inside nasal cavity. CT is superior to both plain radiographs that get adversely affected by superimposition and magnetic resonance imaging which lacks the sensitivity to pick up bony erosions and calcifications. Rhinoliths on CT characteristically appear radio-opaque masses with irregular contours and hypodense or radiolucent core [10].
Primary modality of treatment is removal of the mass. The acceptable approach shall depend upon its location, size and the need to perform secondary procedures. The tools in the armamentarium of an ORL surgeon to tackle this tricky situation include endoscopic endonasal approach, Le Fort I osteotomy, piriform aperture osteotomy, piecemeal removal and lithotripsy [8].
Conclusion
While rhinoliths are an extremely unaccustomed entity, clinicians must be wary of it. The slow growth and subtle or nil symptoms demand a high index of suspicion to facilitate an expeditious diagnosis. History of foreign body introduction may be present only in few cases. It must be a part of differential diagnoses in all cases of unexplained persistent unilateral nasal symptoms like progressive obstruction, fetid rhinorrhea, epistaxis etc. A rigid office nasal-endoscopy complemented with CT facilitates its exact location, disease status of sinuses with the need of secondary surgical procedures. CT can also reveal hidden rhinoliths and is absolutely necessary in planning surgical approach.
Declarations
Authors contributions: ZZ- Data curation, Writing original draft; TM- Writing original draft; VS- Data curation, Formal Analysis, Methodology, Project administration, Supervision, Writing original draft; SG- Radiological images; MGK- Histopathology images; SH- Data curation; VBK- Data curation.
Ethics approval and consent to participate: Approved by the Institutional Ethics Committee, Command Hospital- Kolkata, Alipore Road, Kolkata-700027.
Consent to participate: Informed written consent to participate in the study was taken from the patient.
Consent for publication: Written consent obtained from the patient.
Availability of data and materials: The datasets used and/ or analyzed during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
References
- Kocasarac HD, Celenk P, Erzurumlu Z, Kutlar G. Clinical and radiological aspects of rhinoliths: report of five cases. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. 2013; 116: 232-7.
- Pitt SK, Rout PG. Rhinoliths presenting during routine radiography: two cases. Dental Update. 2000; 27: 505-7.
- Orhan K, Kocyigit D, Kisnisci R, Paksoy CS. Rhinolithiasis: an uncommon entity of the nasal cavity. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2006; 101: e28-32.
- Hadi U, Ghossaini S, Zaytoun G. Rhinolithiasis: a forgotten entity. Otolaryngology-Head and Neck Surgery. 2002; 126: 48-51.
- Appleton SS, Kimbrough RE, Engstrom HI. Rhinolithiasis: a review. Oral surgery, oral medicine, oral pathology. 1988; 65: 693- 8.
- Royal SA, Gardner RE. Rhinolithiasis: an unusual pediatric nasal mass. Pediatric radiology. 1998; 28: 54-5.
- Yildirim N, Arslanoglu A, Sahan M, Yildirim A. Rhinolithiasis: clinical, radiological, and mineralogical features. American journal of rhinology. 2008; 22: 78-81.
- Polson CJ. On rhinoliths. The Journal of Laryngology & Otology. 1943; 58: 79-116.
- Kose OD, Kose TE, Erdem MA, Cankaya AB. Large rhinolith causing nasal obstruction. Case Reports. 2015; 2015: bcr2014208260.
- Tekin I, Fitoz S, Yagci C, Akyar S. Case Report: Rhinolithiasis: Radiologic Findings. Turk J Diagn Intervent Radiol. 2001; 7: 350-2.