
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A case of pneumopericardium
Fatima Lakhani, MD; Victor G Becerra-Gonzales, MD; Sharon Andrade-Bucknor, MD*
Division of Cardiovascular Medicine, University of Miami Miller School of Medicine, USA.
*Corresponding Author : Andrade-Bucknor S
Division of Cardiovascular Medicine, University of
Miami Miller School of Medicine, 1611 NW 12th
Ave, Miami, FL 33136, USA.
Email: s.andradebucknor@med.miami.edu
Received : Jan 14, 2025
Accepted : Feb 05, 2025
Published : Feb 12, 2025
Archived : www.jcimcr.org
Copyright : © Andrade-Bucknor S (2025).
Abstract
Pneumopericardium, defined as air within the pericardial space, is a rare complication associated with trauma and intrathoracic procedures. Here we present a case of a 56-year-old female with chronic myeloid leukemia who recently underwent thoracic surgery admitted for hyperleukocytosis. She was incidentally found to have pneumopericardium on transthoracic echocardiogram and was stable and asymptomatic from a cardiac perspective however underwent a pericardiocentesis for diagnostic purposes, demonstrating a malignant effusion. Although our patient underwent a pericardiocentesis, many cases of pneumopericardium resolve spontaneously, and in asymptomatic patients does not require intervention.
Keywords: Pneumopericardium; Echocardiogram; Thoracic surgery; Chronic myeloid leukemia.
Citation: Lakhani F, Beerra-Gonzales VG, Andrade-Bucknor S. A case of pneumopericardium. J Clin Images Med Case Rep. 2025; 6(2): 3464.
Introduction
Pneumopericardium, the presence of air within the pericardial space, is a rare complication that may occur secondary to intrathoracic procedures, penetrating or blunt chest trauma, and lung infections. Patients may be managed conservatively with close monitoring or by addressing the underlying cause, such as via chest tube placement in the case of an associated pneumothorax [1]. However, in a minority of cases, the accumulation of sufficient air can result in tension physiology, which is potentially life-threatening and requires emergent decompression [1,2]. We report a case of pneumopericardium occurring in the context of recent intrathoracic procedures and recent pneumatosis intestinalis, diagnosed approximately two months prior to presentation.
Case presentation
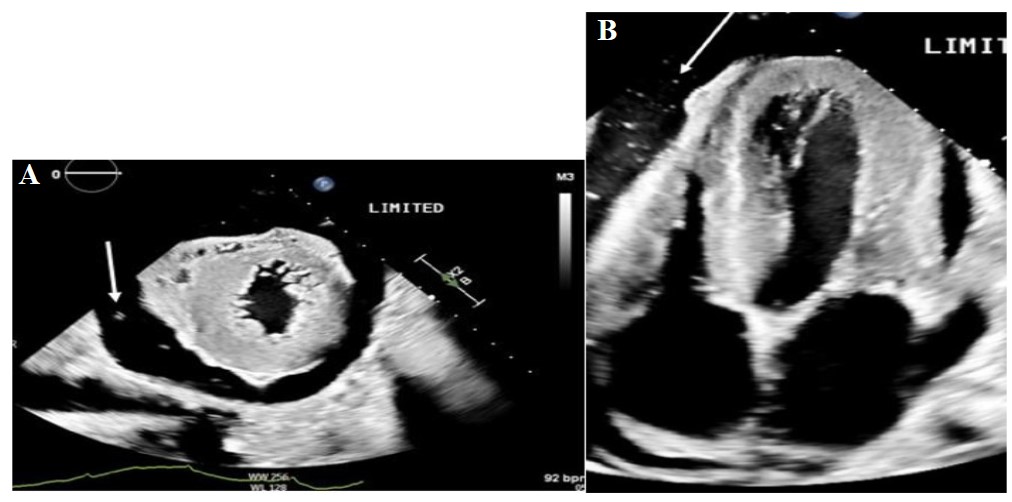
A 56-year-old female with a history of atypical Chronic Myeloid Leukemia (CML) and right upper lobe pulmonary adenocarcinoma presented to the outpatient clinic with shortness of breath and fatigue. She had undergone right robotic thoracoscopy, right upper lobectomy, and complete thoracic lymphadenectomy two months earlier. One month later, a chest tube had been placed due to findings of an empyema/malignant effusion. Laboratory studies completed at the clinic demonstrated significant hyperleukocytosis and she was referred for admission. In the emergency room, she was afebrile and normotensive, blood pressure 122/86 mmHg, with heart rate of 95/min and respiratory rate 25-30/min, O2 saturation was 95% on room air. Physical exam revealed a cachectic, ill-appearing female with decreased breath sounds in both lung bases and bilateral lower extremity edema. Laboratory results included white blood cell count 82,000, platelet count 997,000 and hemoglobin 8.4 g/ dL. Other significant blood tests included uric acid 10.3 mg/ dL, phosphorus 6.6 mg/dL and LDH 1,054. SARS-COV2 was not detected. Chest X-ray showed post-surgical changes compatible with right upper lobectomy, a small right apical pneumothorax and bibasilar opacities. A non-contrast chest CT scan performed that day demonstrated a moderate right and a small left pleural effusion, with compressive atelectasis and loculated fluid and gas within the right upper lobectomy cavity. An abdominal CT showed scattered foci of gas within the small bowel wall consistent with Pneumatosis Intestinalis (PI). Hepatosplenomegaly, splenic infarcts, and ascites were also noted (Figure 1). A Transthoracic Echocardiogram (TTE) done the following day showed normal left ventricular function with an ejection fraction of 60-65% and a large pericardial effusion. Small, bright echodensities were seen in the pericardial fluid, consistent with microbubbles. There was no evidence of tamponade.
Of note, an echocardiogram done 3 weeks earlier had demonstrated only a small to moderate pericardial effusion with no microbubbles. Due to high suspicion for a malignant pericardial effusion, she was referred to cardiothoracic surgery for consideration of a pericardial window. However, given her high surgical risk, pericardiocentesis was performed instead two days later. Immediate follow-up TTE noted only trace pericardial effusion. The pericardial fluid findings included a red blood cell count of 9,000/mm3, white blood cell count of 465/mm3, neutrophil count of 58%, and lymphocyte count of 24%. Cultures were negative; however, flow cytometry demonstrated an abnormal myeloid blast population; CD34 positive myeloid blasts comprised 0.7% of total leukocytes consistent with a myeloid neoplasm. She was treated for tumor lysis syndrome, started on hydroxyurea, and discharged on venetoclax and azacytidine for atypical CML. The next month, a repeat TTE demonstrated a small-moderate effusion without evidence of bubbles. Although the pneumopericardium in this case was successfully treated, unfortunately, the CML proved refractory to treatment. She ultimately developed AML with resultant complications warranting multiple subsequent admissions and succumbed to her illness 6 months later.
Discussion
Pneumopericardium, the presence of air in the pericardial sac, is infrequently encountered. It is most commonly due to a fistula between a cavity such as the pleural space, airways, gastrointestinal tract, or lung abscess and the pericardial space [1]. Etiologies include congenital abnormalities, iatrogenic causes (related to thoracic surgery, epigastric procedures, positive pressure ventilation, central line cannulation), thoracic trauma, severe asthma, and infections such as tuberculosis and HIV [1-3]. Endomyocardial biopsy, pericardiocentesis [6,8] and pacemaker placement [7] have also been implicated among the iatrogenic causes and more recently, cases of spontaneous pneumopericardium have been reported in the setting of COVID- 19 infection [9].
Symptoms may include shortness of breath and sharp chest pain [2]. On examination, the characteristic auscultatory sound referred to as bruit de moulin, which has been attributed to the interaction of air and fluid in the pericardium, may be heard. Electrocardiogram may show evidence of pericarditis, nonspecific ST changes, and low voltages [4]. The “halo sign”, an area of radiolucency surrounding the heart shadow, can be seen on plain radiography and is diagnostic. Associated pneumomediastinum, pneumothorax, or pneumoperitoneum may also be seen radiographically. Subcutaneous emphysema has been described in some cases associated with dental surgery and central venous catheters. CT scans offer further delineation of pneumopericardium and other air collections. TTE findings include the “air gap sign” which refers to changing of the cardiac shape in a cyclic fashion due to the air in the pericardial sac and the “swirling bubbles sign” manifested as small echogenic spots due to the presence of microbubbles at the air-fluid interfaces generated by the movement of the heart [10] as seen in our case. Notably, the halo sign, seen in most cases, was absent in our case and diagnosis was made by echocardiography. An asymptomatic, hemodynamically stable pneumopericardium does not require specific treatment and may resolve spontaneously. However, monitoring for conversion to tension physiology with signs of tamponade is essential. If a tension pneumopericardium is present, immediate decompression is required as mortality rates as high as 50% have been shown [1,2].
Pneumatosis intestinalis refers to extraluminal bowel gas confined within the bowel wall. It is associated with bacterial infections like C. diff, intestinal neoplasms, bowel ischemia, inflammatory or autoimmune bowel disease, immunosuppressive therapy, and mechanical trauma. The occurrence of pneu- mopericardium in conjunction with PI, as seen in this patient, is rare. Extensive thoracic surgery with residual pneumothorax were the most likely inciting factors for the pneumopericardi- um, however, PI and empyema were possible contributors. The etiology of PI found in our patient remains unclear.
Conclusion
Pneumopericardium is defined by air in the pericardial sac. It is often secondary to iatrogenic etiologies, in our case, thoracic surgery. When asymptomatic, patients may be monitored for spontaneous resolution. However, close monitoring is required given the risk of development of tension like physiology which requires urgent decompression.
References
- Anand R, Brooks Md Facs SE, Puckett Y, Richmond RE, Ronaghan CA. Pneumopericardium Resulting from Blunt Thoracic Trauma. Cureus. 2020; 12: e11625.
- Golota JJ, Orlowski T, Iwanowicz K, Snarska J. Air tamponade of the heart. Kardiochir Torakochirurgia Pol. 2016; 13: 150-3.
- Chopra V, Garg N, Mrigpuri P. Spontaneous pneumopericardium an unusual complication in a patient of HIV and pulmonary tuberculosis. Lung India. 2013; 30: 148-50.
- Cummings RG, Wesly RL, Adams DH, Lowe JE. Pneumopericardium resulting in cardiac tamponade. Ann Thorac Surg. 1984; 37: 511-8.
- Gambí Pisonero D, Garrido Menéndez F, Menéndez Sánchez P, Sancho Calatrava E. Neumopericardio secundario a neumatosis quística intestinal: Una complicación infrecuente de una enfermedad rara. Revista Española de Enfermedades Digestivas. 2010; 102.
- Tania Ramírez Martínez, Emilia Blanco Ponce, Marcos García-Guimarães, Gerard Torres, Jara Gayán Ordán, Iatrogenic pneu - mopericardium following pericardiocentesis, European Heart Journal - Cardiovascular Imaging. 2024.
- Enokizono, Kei et al. Very Late-onset Atrial Lead Perforation Leading to Pneumopericardium. Journal of cardiovascular electrophysiology. 2023; 34: 1473–1476.
- Triantafyllis, Andreas S, Tatiana Zamfir, Nestoras Kontogiannis. Pneumopericardium as a Complication of Pericardiocentesis. Canadian Medical Association journal (CMAJ). 2023; 195: E193–E194.
- Figueras R, Yang K, Schurman A, Albini P, Mittal A. 204: Pneumopericardium in Covid-19: A Systematic Review. Critical Care Medicine. 2023; 51: 86-86.
- Pinto TC, Martins T, Seabra D, Moreno N. The “airgap” and “swirling bubbles” signs in a patient with esophageal carcinoma. Echocardiography. 2023; 40: 252–258.