
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A young child with myositis ossificans treated with indomethacin
Zhaohong Yan; Zhidong Li; Mengmeng Xu; Jiaming Zhang; Wendong Yang; Xiaowei Chen*
Department of Rehabilitation Medicine, The First Hospital of Jilin University, China.
*Corresponding Author : Xiaowei Chen
Department of Rehabilitation Medicine, the First
Hospital of Jilin University No.1 Xinmin Street,
Changchun, Jilin 130021, China
Email: cxw0201@jlu.edu.cn
Received : Jan 16, 2025
Accepted : Feb 05, 2025
Published : Feb 12, 2025
Archived : www.jcimcr.org
Copyright : © Xiaowei C (2025).
Abstract
Heterotopic Ossification (HO) refers to the abnormal formation of bone tissue in locations other than the skeleton. When abnormal bone deposits occur within muscles, it is called Myositis Ossificans (MO), and when it occurs in soft tissues, it is often referred to as HO [19]. Acquired HO mainly occurs after trauma, spinal cord injury, and soft tissue injury, and it is mainly related to local trauma, prolonged compression, or inappropriate postoperative rehabilitation [19]. A study showed that the ossification of soft tissues such as skeletal muscles in older people may be a new marker of aging [3]. The incidence of HO in adults varies greatly among research centers, ranging from 24% to 42% [4,7]. However, in complex diseases, such as fractures combined with traumatic brain injuries, the incidence of HO is 46.0%, which is higher than that in simple fractures (26.3%) [9]. In children, the incidence of HO is relatively low, ranging from 4% to 22% [13]. HO often presents as localized swelling and pain in the affected area, which may lead to limited motor function and, in severe cases, affect daily living activities. Common sites in children include the elbow and knee joints, which are more prone to injury during exercise and activities. As regards treatment, early identification and intervention are very important. The most commonly used drugs are Nonsteroidal Anti-Inflammatory Drugs (NSAIDs), such as indomethacin. However, no studies have reported on the use of indomethacin in children.
In the case presented, the patient was an 8-year-old girl who suffered from secondary MO near the elbow joint due to improper rehabilitation after elbow joint fracture surgery. She was treated with indomethacin for 2 months and achieved satisfactory results without any adverse reactions.
Keywords: Myositis ossificans; Indomethacin; Pediatrics; Elbow joint fracture; Postoperative joint stiffness; Rehabilitation.
Citation: Zhaohong Y, Zhidong L, Mengmeng X, Jiaming Z, Xiaowei C. A young child with myositis ossificans treated with indomethacin. J Clin Images Med Case Rep. 2025; 6(2): 3465.
Clinical case
The patient was an 8-year-old girl (weight, 40 kg). The main complaint was “limited elbow joint movement with swelling and pain” for >2 months. The patient suffered a right supracondylar fracture of the humerus after falling on August 13, 2023. She received surgical treatment and underwent rehabilitation after the removal of Kirschner wires 6 weeks after surgery. During this period, she experienced a local increase in skin temperature, swelling, and pain in the right elbow joint. No medication or physical agent modality was given, and after a brief rest, rehabilitation continued. However, the pain and swelling per- sisted. The patient had no special medical history. On her visit to the clinic 10 weeks after surgery, she presented with pain, increased skin temperature, swelling in the right elbow joint, limited Range of Motion (ROM), and passive ROM (PROM) of 30°-90° in the elbow joint. X-ray imaging of the right elbow joint revealed an irregular high-density area around the proximal of the right ulna. Combined with the medical history, she was diagnosed with MO.
She received the following treatment: oral administration of indomethacin at 2.5 mg/kg, three times a day; physical agent modality of laser therapy, 20 min, once a day; medium-frequency electrical therapy, 15 min, once a day; physical therapy with Maitland joint mobilization technique levels 1 and 2 to relieve elbow pain, 2 min at a time, 5 times per group, 2 groups per day; fascia manipulation to relax the biceps brachii, triceps brachii, and soft tissues around the elbow joint, 2 min at a time, 2 times per group, 2 groups per day; muscle strength training, including elbow wrist flexion and extension and forearm rotation muscle groups, 10 times per group, 2 groups per day; strictly control of pain and swelling during treatment; and gradually increasing functional training and endurance training.
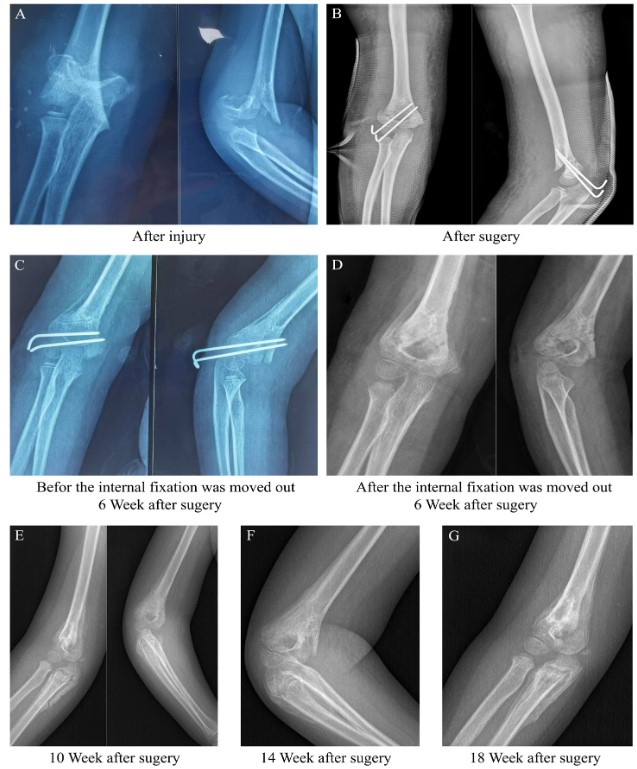
Fourteen weeks after surgery, the skin temperature returned to normal, swelling disappeared, and the PROM of the right elbow increased to 5°-125°. X-ray imaging showed complete ossification and a stable fit with the ulna. Laboratory examination revealed normal levels of calcium, phosphorous, and alkaline phosphatase (an indicator of HO stability). The patient was asked to stop taking indomethacin. During the treatment period, the patient did not experience any adverse reactions from taking NSAIDs. Eighteen weeks after surgery, the PROM of the right elbow returned to normal. The evolution of ossification under X-ray imaging is shown in (Figure 1).
Discussion
MO often occurs in the quadriceps femoris, biceps brachii, triceps brachii, etc [10]. Its pathogenesis is still unclear; at present, it is mainly believed to be related to posttraumatic local inflammatory response, immune system disorder, and hypermetabolism. When local tissue is damaged, acute inflammation promotes the formation of ossification, and macrophages promote bone formation by expressing high levels of the osteogenic growth factor BMP4. In addition, the increase in mast cells may cooperate with macrophages to induce the ossification. The immune system also affects osteoclast production, which is an important step in the formation of ectopic ossification [10]. Based on the pathogenesis, the existing NSAID therapy for prevention is still the preferred option, which mainly inhibits the formation of prostaglandins and the progression of osteoblasts’ cell cycle [2,15]. Patients aged >15 years are recommended to start taking indomethacin after surgery, 25 mg/day, three times a day, until 6 months [15]. Clinical studies have found that the preventive use of NSAIDs has significantly reduced the incidence of HO after surgery [15,17]. However, a study reported that NSAIDs have no significant preventive effect on HO [12]. Although indomethacin has been widely used in adults to prevent HO [1,18] no experience has been reported on the use of indomethacin in patients aged <15 years.
The patient had a circumscribed MO after undergoing inappropriate physical therapy following elbow surgery. The patient suffered from muscle strain in the forearm muscle group, which subsequently led to MO formation. The age range of onset for circumscribed MO is 20-30 years [16]. In the early stage, it may be manifested as increased skin temperature, swelling, and limited ROM of nearby joints, which is consistent with the clinical presentation of this case. In the early stage, MO should be differentiated from other diseases such as extraskeletal osteochondroma, nodular fasciitis, and calcified aponeurotic fibroma [22]. According to the Hastings and Graham classification [8], the patient had grade I MO, with obvious heterotopic ossification; however, the activity of the elbow joint was not affected. For the child’s elbow pain, increased skin temperature, and swelling, laser and medium-frequency electrotherapy were used to reduce local inflammatory reactions while also administering oral indomethacin. Owing to the lack of experience in indomethacin therapy in children with MO, we referenced the recommendations on the safe dosage for patients aged 2-15 years with rheumatic diseases [21]. In this case, the child was administered indomethacin 2 mg/kg/day in three divided doses for a total of 2 months. MO stabilized without progression, and no new ossifications formed. The markers of the HO maturation of alkaline phosphatase returned to normal [5]. The child did not report any adverse effects during the medication period, indicating that the indomethacin dose is safe for use in young children with MO.
In addition, to drug therapy, MO can be treated with radiation and surgery. Radiotherapy is rarely used in children, whereas surgery is generally applied in patients with severe pain, ineffective oral analgesics, and severe joint movement restrictions. Performing surgery after 1 year is recommended to avoid recurrence [13]. With the deepening of research on MO, some new strategies have also been applied to HO [6,11,14,20]. However, further research on their efficacy is still needed. MO is a self-limiting disease that will naturally stop progressing after a period. In individual cases, ossification will naturally absorb within a few months to a few years. A study reported that after treatment with palovarotene, not only the volume of the newly formed ossification decreased but also the existing ossification showed signs of being absorbed in some patients [14].
Conclusion
For patients with postoperative joint stiffness, physical therapy involving intense activities should be avoided, particularly in patients with muscle strain and swelling. Physical agent modalities and NSAIDs should be given promptly to prevent the formation of myositis ossification. Early intervention and individualized treatment are crucial for pediatric MO, and indomethacin could be used for the treatment of pediatric MO.
References
- Atwan Y, Abdulla I, Grewal R, Faber KJ, King GJK, Athwal GS. Indomethacin for heterotopic ossification prophylaxis following surgical treatment of elbow trauma: a randomized controlled trial. J Shoulder Elbow Surg. 2023; 32: 1242-1248.
- Banovac K, Williams JM, Patrick LD, Haniff YM. Prevention of heterotopic ossification after spinal cord injury with indomethacin. Spinal Cord 2001; 39: 370-374.
- Dai GC, Wang H, Ming Z, Lu PP, Li YJ, Gao YC, et al. Heterotopic mineralization (ossification or calcification) in aged musculoskeletal soft tissues: a new candidate marker for aging. Ageing Res Rev. 2024; 95: 102215.
- Douglas K, Cannada LK, Archer KR, Dean DB, Lee S, Obremskey W. Incidence and risk factors of heterotopic ossification following major elbow trauma. Orthopedics. 2012; 35: e815-822.
- Eekhoff EMW, Botman E, Netelenbos JC, Graaf Pd, Bravenboer N, Micha D, et al. [18F] NaF PET/CT scan as an early marker of heterotopic ossification in fibrodysplasia ossificans progressiva. Bone. 2018; 109: 143-146.
- Felix-Ilemhenbhio F, Pickering GAE, Kiss-Toth E, Wilkinson JM. Pathophysiology and emerging molecular therapeutic targets in heterotopic ossification. Int J Mol Sci. 2022; 23: 698.
- Forsberg JA, Pepek JM, Wagner S, Wilson K, Flint J, Andersen RC, et al. Heterotopic ossification in high-energy wartime extremity injuries: prevalence and risk factors. J Bone Joint Surg Am. 2009; 91: 1084-1091.
- Hastings H 2nd, Graham TJ, The classification and treatment of heterotopic ossification about the elbow and forearm. Hand Clin. 1994; 10: 417-437.
- Jodoin M, Rouleau DM, Therrien E, Chauny JM, Sandman E, Larson-Supuis C, et al. Investigating the incidence and magnitude of heterotopic ossification with and without joints involvement in patients with a limb fracture and mild traumatic brain injury. Bone Rep. 2019; 11: 100222.
- Kraft CT, Agarwal S, Ranganathan K, Wong VW, Loder S, Li J, et al. Trauma-induced heterotopic bone formation and the role of the immune system: a review. J Trauma Acute Care Surg. 2016; 80: 156-165.
- Lees-Shepard JB, Goldhamer DJ. Stem cells and heterotopic ossification: lessons from animal models. Bone. 2018; 109: 178-186.
- Leyder D, Döbele S, Konrads C, Histing T, Fischer CS, Ahrend MD, et al. Classification and incidence of heterotopic ossifications in