
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Cutaneous lupus erythematosus and lichen planus overlap syndrome: A case report
Gardenia Akhyar; Aisha Triani*; Rina Gustia; Irdawaty Izrul; Mutia Sari
Department of Dermatology and Venereology, Faculty of Medicine, Andalas University, Padang, Indonesia.
*Corresponding Author : Aisha Triani
Department of Dermatology and Venereology,
Faculty of Medicine, Andalas University, Padang,
Indonesia.
Email: aishariani24@gmail.com
Received : Jan 16, 2025
Accepted : Feb 06, 2025
Published : Feb 13, 2025
Archived : www.jcimcr.org
Copyright : © Triani A (2025).
Abstract
Background: The convergence of Cutaneous Lupus Erythematosus (CLE) and Lichen Planus (LP) into an overlapping syndrome represents a rare medical phenomenon, characterized by distinct pathological mechanisms. This syndrome exhibits unique clinical and histopathological features that mirror those of both lupus erythematosus and lichen planus. The impact of these lesions is widespread, affecting regions ranging from the face and scalp to the arms, legs, and trunk. Clinically, the cutaneous manifestations manifest as multiple pruritic to painful erythematous-violaceous thickened plaques, slightly scaly in nature, with a central area of atrophy. In addition, ulcerated plaques and a reticulated form have been observed in the buccal mucosa.
Case presentation: A 63-year-old Indonesian man who had previously been diagnosed with hypertrophic lichen planus a year earlier. In this instance, he experienced a worsening of symptoms, characterized by exacerbated pruritic erythematous-violaceous thickened plaques displaying central atrophy. To ascertain the diagnosis, the patient underwent both dermoscopy examinations and skin biopsies across six distinct areas. The results from these assessments consistently indicated the presence of the LE/LP overlap syndrome. For treatment, the patient underwent a six-week oral steroid taper regimen, along with antihistamines and topical steroids followed by emollient therapy. Subsequent to three months of this treatment protocol, noticeable improvement was observed.
Conclusion: Correlation between clinical symptoms, dermoscopy examination and histopathological examination is needed to make a diagnosis of cutaneous lupus erythematosus-lichen planus overlap syndrome. Complete documentation of this certain entities is still needed to further explore this disorder.
Keywords: Cutaneous lupus; Lichen planus; Overlap; Dermoscopy.
Citation: Akhyar G, Triani A, Gustia R, Izrul I, Sari M. Cutaneous lupus erythematosus and lichen planus overlap syndrome: A case report. J Clin Images Med Case Rep. 2025; 6(2): 3466.
Introduction/background
Lupus erythematosus/lichen planus overlap syndrome is a rare disorder combining the clinical, histological and immunopathological features of both Lupus Erythematosus (LE) and Lichen Planus (LP). It is consider an elusive entities. Cutaneous lesions mostly affect the distal arms, legs, face and trunk. Palmoplantar involvement is felt to be characteristic of this condition. Plaques are often painful, centrally atrophic, bluish-red to hypopigmented in color, large, and scaly. The etiology is largely unknown, but its possibilities include an autoimmune, viral, and/or genetic cause. Drugs that may induce LE/LP overlap syndrome are isoniazid, procainamide, and acebutolol [2,3]. The exact incident for this disease remains unknown.
Approximately 50 cases of LE/LP overlap syndrome have been reported so far. Of those cases, mainly two different types of lesions have been described: (i) painful, bluish red, scaly centrally atrophic plaques, occurring primarily on the extremities, and (ii) verrucous, papulonodular lesions on the hands and arms. However, cutaneous lesions located on different sites, including the face, trunk, mucosa and nails have been reported [2]. Complete documentation of this certain entities is needed to further explore this disorder.
Case presentation
A 63-year-old man with complaints of purplish-red itching on the patient’s face, lips, scalp, chest, back, and both arms and hands which has been getting wider since 2 months ago. One year earlier the patient has a history of being diagnosed with hypertrophic lichen planus in both arms and at the back of his hand since 1 year ago, the patient has received treatment and has been treated to show some improvement. Physical examination reveals multiple purple-red discoid lesions, with atrophic center and hyperpigmented margins and fine white scales on the cheek, lips, chest, and upper back. While in both lower arms and the back of the hand there are polygonal violaceous papules that felt itchy.
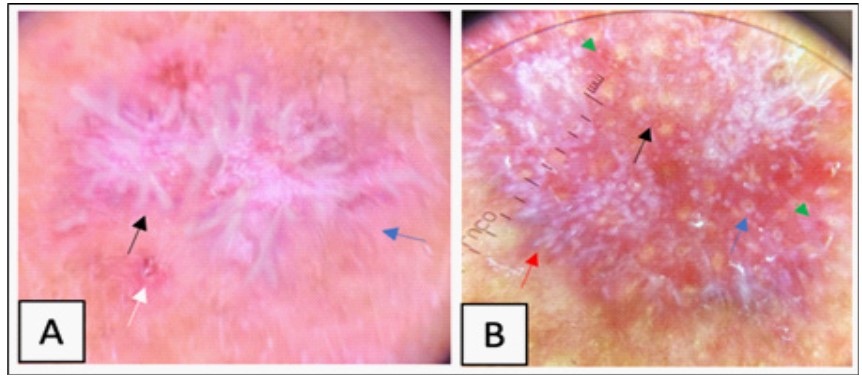
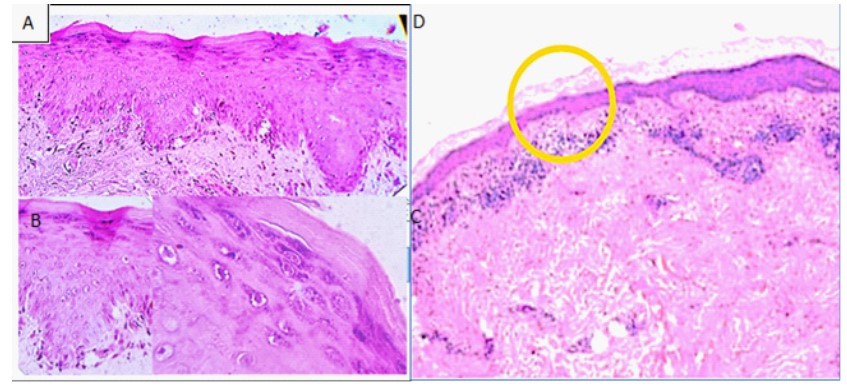
Dermoscopy in the lesion in area cheek, lips, chest and upper back showed perifoilular plug, perifollicular whiteish halo, starburst pattern, and multiple follicular red dots. While on the lesion in patient’s lower arms and the back of the hand showed wickem’s striae (Figure 2). We also take biopsies from lesion in six location, hystopatologi examination from lesion both arms were found that there was an interface reaction of epidermal dermatitis with hyperkeratosis, areas of hypergranulosis, and a picture of hydrophilic degeneration in the basal epidermis. Saw the presence of saw tooth on the rete ridge and colloid bodies (civatte bodies) in the epidermis. In the dermis, infiltrate lymphocytes, histiocytes that form bands and macrophages contain pigment, suggesting lichen planus (Figure 3).

Discussion
Cutaneous lupus erythematosus and lichen planus overlap syndrome is a rare disorder combining the clinical, histological and immunopathological features of both Lupus Erythematosus (LE) and Lichen Planus (LP). Cutaneous lesions mostly affect the distal arms, legs, face and trunk. Plaques are often painful, centrally atrophic, bluish red to hypopigmented in color, large, and scaly. On biopsy of clinically ambiguous lesions, histopathological features of one or both processes can be found, obscuring the diagnosis and complicating prognosis and treatment [1,2].
The majority of cases occurs between the ages of 25 to 45 with a slight female predominance. Cutaneous lesions mostly affect the distal arms, legs, face and trunk. The etiology is largely unknown, but its possibilities include an autoimmune, viral, and/or genetic cause. Drugs that may induce LE/LP overlap syndrome are isoniazid, procainamide, and acebutolol [2,3]. The exact incident for this disease remains unknown. Literatures suggests only around 50 cases ever reported of this condition. Therefore, establishing the diagnosis is still a challenging matter. This is the first case report of cutaneous lupus erythematosus and lichen planus overlap syndrome in our hospital.
Schmitz reported one case of a 70-year-old Caucasian man with an exacerbation of a pruritic skin eruption present on-and-off for seven years. The patient had three previous skin biopsies between 2011 and 2014 consistent with LP. As in this case, the diagnosis of LE or LP-LE overlap syndrome may require multiple biopsies to be performed or for other constitutional signs of LE to be present. Once the diagnosis was established as LP-LE overlap syndrome, the patient was adjusted to receive the appropriate treatment of oral prednisone, and hydroxychloroquine, he showed improvement [3].
Tursen in Turkey reported a 34-year-old woman presented with skin and mucosal lesions of nine years duration. On dermatological examination, she had violaceous, thickened, scaly lesions on scalp, arms, malar and auricular regions and her buccal and lip mucosa showed white papules with a reticular pattern, the patient also had an erythematous, well-defined, mildly raised plaque on her left lower eyelid involving one-third of the lateral portion. Prescribed hydroxychloroquine 200 mg orally twice daily. The eyelid, mucosal and skin lesions improved dramatically within two weeks. The therapy was gradually tapered over six months, and the patient is still free of symptoms [8].
Lupus erythematosus and lichen planus are well established and distinct entities, but cases arise in which the two conditions coexist or cannot be readily distinguished from one another but is recently referred to as LE/LP overlap syndrome. Now also including the former condition. In some cases of the overlap syndrome, the histological features and Direct Immunofluorescent (DIF) are more consistent with LP, while in other cases with LE. In yet another subset of patients, the lesions of LE and LP coexist, rather than overlap, raising the controversial issue of the authenticity of LE/LP overlap syndrome. Interestingly, in addition to distinct lesions of LE and LP, our case presented a lesion with combined features of LE and LP that was confirmed by both histopathological and immunofluorescence studies. It appears that our case represents a true form of “overlapped” LE and LP [4,10].
Unfortunately, in our patient, we are unable to perform the Direct Immunofluorescent (DIF) due to the unavailability of such examination in our center. We are also having difficulty sending the sample to another center due to transport issue.
As is true in clinical features, histopathological findings usually enable us to draw the distinction between LE and LP in most cases, although they may be of some difficulty in less typical or overlapping cases. Because characteristic immunoglobulin deposits are known to be found in the skin lesions of LE and LP, DIF studies are known to be helpful in distinguishing between the two diseases. In LE, immunoglobulins (IgG, IgA and IgM) and complement components deposited in a continuous granular line or band along the dermo-epidermal junction have been observed [2,4,10].
Our patient’s disease had previously been diagnosed in its earlier stages as lichen planus prior to presentation to Dermatology and we believe that this condition may be underreported in the population. This may be due to disease course from chronic cutaneous LE and variant of hypertrophic LP as it happened at the same time. This rare case highlights the unique co-existence of both conditions resulting in a syndrome. It is also show remarkable result with first line treatment of steroid therapy.
Conclusion
A case of typical LE/LP overlap syndrome is reported, Clinical descriptions of LE-LP overlap syndrome vary widely, ranging from typical, flat-topped papules, as seen in lichen planus, to atrophic scaling plaques, more reminiscent of Discoid Lupus Erythematosus (DLE). The diagnosis is based primarily on the combined presence of clinical, histologic, and/or immunologic features of both diseases occurring at the same time. Predominantly reported to coexist with DLE. Although this case appears to be manageable with first-line treatment. Thorough documentation of this certain entities is still needed to further explore this particular disorder.
References
- Lospinoso D, Fernelius C, Edhegard K, Finger D, Arora N. Lupus erythematosus/lichen planus overlap syndrome: successful treatment with acitretin. Lupus. 2013; 22: 851–854.
- Demirci GT, Altunay IK, Sarıkaya S, Sakiz D. Lupus erythematosus and lichen planus overlap syndrome:a case report with a rapid response to topical corticosteroid therapy. Dermatology reports. 2011; 3: e48.
- Schmitz S, Vatanchi M, Alapati U. Seven-year itch: a perplexing case of lichen planus-lupus erythematosus overlap syndrome. Dermatology Online Journal. 2018; 24.
- Nagao K, Chen, KR. A case of lupus erythematosus/lichen planus overlap syndrome. The Journal of Dermatology. 2006; 33: 187–190.
- De Jong, MGJ, van de Kerkhof. Coexistence of palmoplantar lichen planus and lupus erythematosus with response to treatment using acitretin. British Journal of Dermatology. 1996; 134: 538–541.
- Inaloz H, Chowdhury M, Motley R. Lupus erythematosus/lichen planus overlap syndrome with scarring alopecia. Journal of the European Academy of Dermatology and Venereology. 2001; 15: 171–174.
- Camisa C, Neff JC, Olsen RG. Use of indirect immunofluorescence in the lupus erythematosus/lichen planus overlap syndrome: An additional diagnostic clue. Journal of the American Academy of Dermatology. 1984; 11: 1050–1059.
- Tursen U, Oz O, Íkizoglu G, Kaya TI, Dusmez D. A Case of Lichen Planus-Lupus Erythematosus Overlap Syndrome with Eyelid Involvement. European Journal of Ophthalmology. 2002; 12: 244– 246
- Ioannides D, Vakirlis E, Kemeny L, Marinovic B, Massone C, Murphy R, et al. European S1 guidelines on the management of lichen planus: a cooperation of the European Dermatology Forum with the European Academy of Dermatology and Venereology. 2020
- Smirnov B, Bowles AA, Strasswimmer JM, Nousari CH. Lupus Erythematosus Lichen Planus Overlap Syndrome Mimicking Squamous Cell Carcinoma. The Journal of clinical and aesthetic dermatology. 2019; 12: 36–38.