Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Rare catastrophic complication of thoracic aneurysms
Billurvan Taskin*; Daniel Vogele
Department of Radiology and Interventional Radiology, University Hospital ULM, Germany.
*Corresponding Author : Billurvan Taskin
Department for Radiology and Interventional
Radiology, University Hospital ULM, Albert-Einstein-
Allee 23, 89081 Ulm, Germany.
Email: billurvan.taskin@uniklinik-ulm.de
Received : Jan 20, 2025
Accepted : Feb 06, 2025
Published : Feb 13, 2025
Archived : www.jcimcr.org
Copyright : © Taskin B (2025).
Citation: Taskin B, Vogele D. Rare catastrophic complication of thoracic aneurysms. J Clin Images Med Case Rep. 2025; 6(2): 3467.
Description
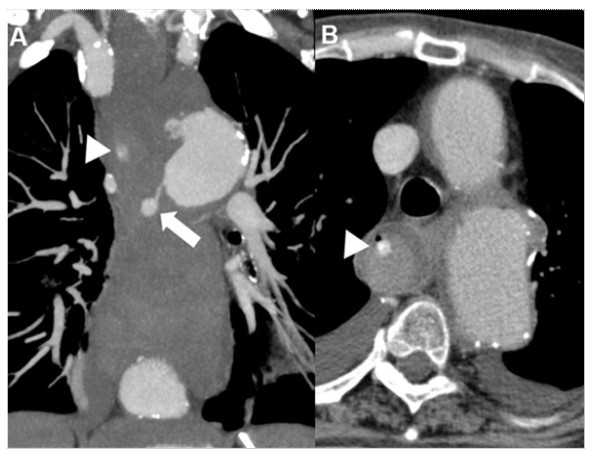
A 69-year-old patient with a thoracic aortic aneurysm (~9 cm) developed hemodynamically significant hematemesis a few days before surgery. Computed Tomography (CT) revealed an Aorto-Esophageal Fistula (AEF) (Figure 1). Despite emergency Thoracic Endovascular Aortic Repair (TEVAR), the patient died in hemorrhagic shock. An AEF is an extremely rare complication of thoracic aortic aneurysms or after aortic interventions. If left untreated it’s 100% lethal, perioperatively up to 77%. The absence of early specific symptoms is challenging for accurate early diagnosis. The so-called “Chiari triad” is sometimes described: initial chest pain, dysphagia, hematemesis or melena with exsanguination after an asymptomatic interval. In cases of such clinical findings or gastroscopic pulsatile mass, an AEF should be considered; in those cases deep biopsies are prohibited and CT-Angiography should be performed. An AEF with massive hemorrhage requires multidisciplinary management. Typically, a Sengstaken-Blakemore tube can be placed, followed by TEVAR for bleeding control before definitive aortic repair/ reconstruction.