
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Pituitary stalk interruption syndrome: Clinical and imaging insights
Beqqali Basma, MD*; Imrani Kaoutar, PhD; Dghoughi Basma, MD; Boutaleb Joud, MD, Kabila Badr, MD; Moatassim Billah Nabil, PhD; Nassar Intissar, PhD
Central Radiology Department, IBN SINA University Hospital V, Rabat, Morocco
*Corresponding Author : Beqqali Basma, MD
Central Radiology Department, IBN SINA University
Hospital V, Rabat, Morocco.
Tel: +212667799987
Email: beqqali.basma@gmail.com
Received : Jan 13, 2025
Accepted : Feb 07, 2025
Published : Feb 14, 2025
Archived : www.jcimcr.org
Copyright : © Basma B (2025).
Abstract
Pituitary Stalk Interruption Syndrome (PSIS) is a rare congenital disorder characterized by an absent or interrupted pituitary stalk, an ectopic posterior pituitary, and hypoplasia of the anterior pituitary. It often presents with varying degrees of pituitary hormone deficiencies, leading to growth disorders and reproductive dysfunction. This case report describes a 20-year-old female presenting with primary amenorrhea and hypothyroidism, ultimately diagnosed with PSIS through hormonal evaluation and MRI findings. The case underscores the importance of imaging in confirming the diagnosis and the necessity of hormone replacement therapy for management.
Citation: Basma B, Kaoutar I, Basma D, Joud B, Badr K, et al. Pituitary stalk interruption syndrome: Clinical and imaging insights. J Clin Images Med Case Rep. 2025; 6(2): 3469.
Introduction
Pituitary Stalk Interruption Syndrome (PSIS) is a congenital anomaly resulting in disrupted hypothalamic-pituitary signaling pathways. The syndrome is frequently associated with Combined Pituitary Hormone Deficiencies (CPHD), leading to clinical manifestations such as short stature, growth hormone deficiency, and reproductive dysfunction. The underlying etiology of PSIS remains unclear, but genetic mutations and perinatal injuries have been proposed as contributing factors. MRI serves as the gold standard for diagnosis, revealing the characteristic triad of anterior pituitary hypoplasia, an absent or thin pituitary stalk, and an ectopic posterior pituitary. Early recognition and management with hormone replacement therapy are crucial to preventing long-term complications.
Case report
A 20-year-old female presented for evaluation of primary amenorrhea and hypothyroidism. Her past medical history was unremarkable, with no prior hospitalizations or surgeries, and no family history of endocrine or genetic disorders. She had developed normally through childhood and adolescence without delays in growth or development. Her height was 1.65 m, with a target familial height of 1.70 m, and her weight and BMI were within normal limits. Physical examination revealed normal secondary sexual characteristics, including breast development, but she reported no history of menarche. No facial dysmorphia, skin pigmentation changes, or other abnormalities were noted, and all other aspects of her examination were unremarkable.
Initial laboratory tests revealed hyponatremia, with serum sodium at 120 mmol/L, prompting an endocrine evaluation. Further testing showed low 8 am. cortisol levels (75 nmol/L, normal >138) and ACTH at 13 pg/mL, raising suspicion for Anterior Pituitary Insufficiency (API) [1,2]. A comprehensive hormonal panel confirmed API, as insulin tolerance testing revealed undetectable cortisol and Growth Hormone (GH) levels during hypoglycemia, consistent with a complete pituitary hormone deficiency. Gonadotropin levels were markedly low, with LH <0.1 IU/L (normal 1.7-8.6) and FSH at 0.3 IU/L (normal 1.5-12.4), suggesting hypogonadotropic hypogonadism. Thyroid function tests showed decreased free T4 at 10 pmol/L (normal 12-22) and a suppressed TSH at 0.07 mIU/L (normal 0.27-4.20). Prolactin levels were within the normal range (15 ng/mL).
Given these findings, Magnetic Resonance Imaging (MRI) of the brain and pituitary region was performed. The MRI revealed the classic triad associated with PSIS: a hypoplastic anterior pituitary, an interrupted or absent pituitary stalk, and an ectopic posterior pituitary located above the sella turcica, displaying T1 hyperintensity with post-contrast enhancement. These imaging features confirmed the PSIS diagnosis, a congenital abnormality often resulting in combined pituitary hormone deficiencies due to disrupted hypothalamic-pituitary signaling pathways [1,3,4].
Following diagnosis, the patient was started on hormone replacement therapy with levothyroxine to manage hypothyroidism, and hydrocortisone to address cortisol insufficiency. The hydrocortisone treatment effectively corrected her hyponatremia. Further hormone replacement and regular follow-up were planned to monitor her hormone levels and manage potential complications related to PSIS. This case underscores the critical role of MRI in diagnosing PSIS and highlights the importance of individualized hormone replacement therapy to manage the patient’s symptoms and prevent complications associated with pituitary hormone deficiencies [2].
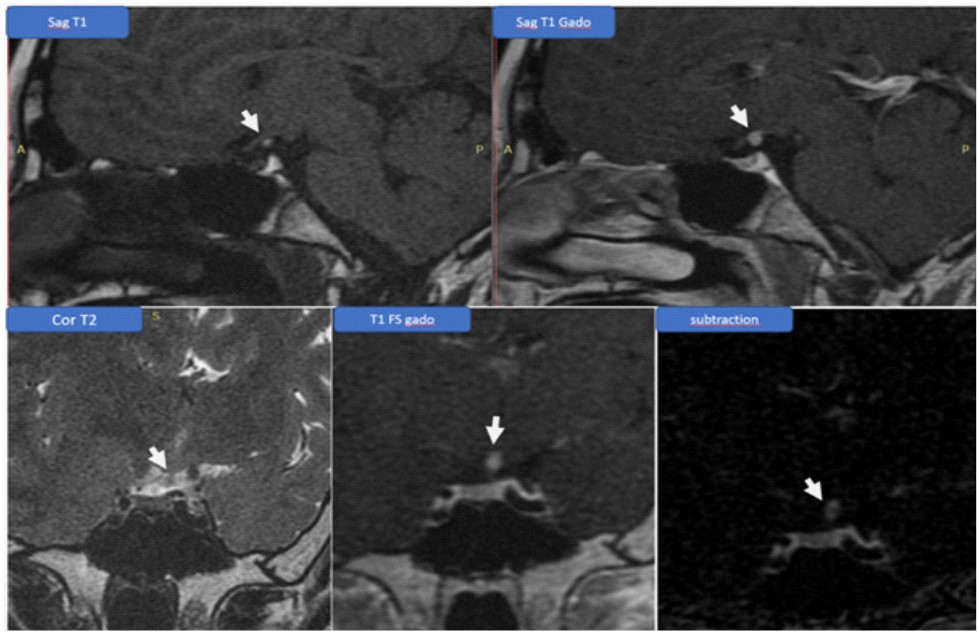
→ Anterior pituitary hypotrophy: Underdevelopment or reduced size of the anterior pituitary gland.
→ Very thin pituitary stalk: Indicates a significantly reduced or barely visible pituitary stalk, which may be associated with compromised hormone signaling.
→ Absence of visible intra-sellar posterior pituitary: The posterior pituitary is not distinguishable within the sella turcica, the usual location.
→ Ectopic supra-sellar posterior pituitary: The posterior pituitary is located above the sella turcica, showing high signal intensity on T1-weighted imaging and enhancement post-contrast injection.
Discussion
PSIS is a rare but significant congenital disorder that can lead to severe endocrine dysfunctions. The etiology of PSIS remains largely unknown, but it is suspected to result from genetic mutations or perinatal insults such as birth asphyxia or breech deliveries. Studies have demonstrated that mutations in genes such as PROP1, LHX3, and OTX2 can contribute to the development of this syndrome [5,6].
Clinically, patients with PSIS can present with a wide spectrum of endocrine deficiencies, ranging from isolated growth hormone deficiency to panhypopituitarism. The severity of hormone deficiencies often correlates with the degree of pituitary stalk interruption, as observed in MRI studies. In our case, the patient exhibited a complete deficiency of anterior pituitary hormones, necessitating lifelong hormone replacement therapy [7].
MRI remains the cornerstone of PSIS diagnosis, providing clear visualization of the pituitary gland’s morphological anomalies. The classic triad seen in MRI—hypoplastic anterior pituitary, absent or interrupted pituitary stalk, and ectopic posterior pituitary—strongly suggests the diagnosis and helps differentiate PSIS from other causes of hypopituitarism. Early MRI evaluation is therefore essential in patients with unexplained growth delay or reproductive disorders [8].
Management of PSIS primarily involves hormone replacement therapy tailored to the patient’s specific deficiencies. Growth hormone therapy, if initiated early, can significantly improve height outcomes in affected individuals. Additionally, timely initiation of cortisol and thyroid hormone replacement is crucial in preventing life-threatening complications such as adrenal crisis. Long-term follow-up is necessary to monitor hormonal levels and adjust treatment accordingly.
Conclusion
Pituitary stalk interruption syndrome is a rare but significant congenital disorder requiring early recognition and intervention. MRI remains the key diagnostic tool for identifying its characteristic triad, allowing for appropriate clinical management. Hormone replacement therapy plays a fundamental role in preventing complications and improving the quality of life of affected individuals. This case highlights the need for increased awareness among clinicians to ensure timely diagnosis and treatment.
Declarations
Conflict of interest: The author(s) declare that they have no conflicts of interest that could have inappropriately influenced them in the writing of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval: No ethical approval was required for this article
Informed consent: Written informed consent was obtained from the patient for the anonymized information to be published in this article.
Guarantor: Beqqali Basma.
References
- Vikas C, Bano S. Imaging in short stature: Pituitary stalk interruption syndrome. Indian Journal of Endocrinology and Metabolism. 2012; 16: 692-697.
- Nawaz A, Azeemuddin M, Shahid J. Pituitary stalk interruption syndrome presenting in a euthyroid adult with short stature. Radiology Case Reports. 2018; 13: 503-506.
- Mirica A, et al. Pituitary stalk interruption syndrome: A clinical case report. Presented at the European Congress of Endocrinology. Endocrine Abstracts. 2021; 73: EP143.
- Wang W, et al. Relationship between pituitary stalk visibility and hormone deficiencies in PSIS. Clinical Endocrinology. 2015; 83: 369-376.
- Wang CZ, Guo LL, Han BY, Su X, Guo QH, Mu YM. Pituitary Stalk Interruption Syndrome: From Clinical Findings to Pathogenesis. J Neuroendocrinol. 2017; 29.
- Julia Vergier, Frederic Castinetti, Alexandru Saveanu, Nadine Girard, Thierry Brue, Rachel Reynaud, DIAGNOSIS OF ENDOCRINE DISEASE: Pituitary stalk interruption syndrome: etiology and clinical manifestations, European Journal of Endocrinology. 2019; 181: R199–R209.
- G Pinto, I Netchine, ML Sobrier, F Brunelle, JC Souberbielle, R Brauner. Pituitary Stalk Interruption Syndrome: A Clinical-Biological-Genetic Assessment of Its Pathogenesisd, The Journal of Clinical Endocrinology & Metabolism. 1997; 82: 3450–3454.
- Gosi SK, et al. BMJ Case Rep. 2019; 12: e230133.