
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Congenital jugular vein phlebectasia: Benign vascular malformation
Isabel Coelho*; Francisca Manoel; Carlota Lopes; José Maria Lupi; Susana Gomes
Department of Pediatrics, Women’s and Children’s Unit, Hospital do Espírito Santo de Évora, Portugal.
*Corresponding Author : Isabel Coelho
Department of Pediatrics, Women’s and Children’s
Unit, Hospital do Espírito Santo de Évora, Portugal.
Email: ivcoelho@hevora.min-saude.pt
Received : Jan 24, 2025
Accepted : Feb 12, 2025
Published : Feb 19, 2025
Archived : www.jcimcr.org
Copyright : © Coelho I (2025).
Abstract
Jugular Vein Phlebectasia is a benign cause for cervical mass in pediatric patients. Usually asymptomatic and of idiopathic origin it can be diagnosed with ultrasound. Conservative treatment is usually advised if no symptoms or psycological concerns are present. Albeight rare, its benign course warrants knowledge to avoid unnecessary interventions.
Keywords: Vascular malformation; Jugular veins; Congenital abnormalities; Ultrasonography.
Citation: Coelho I, Manoel F, Lopes C, Lupi JM, Gomes S. Congenital jugular vein phlebectasia: Benign vascular malformation. J Clin Images Med Case Rep. 2025; 6(2): 3475.
Clinical presentation
A 3-year-old boy with no significant past medical history presented to the emergency department for evaluation of acute nasopharyngitis. On observation, a pulsatile left lateral cervical mass was noted (Figure 1). The boy’s mother reported the presence of this mass since birth, with no associated symptoms or history of recurrent infections, trauma or previous surgery.
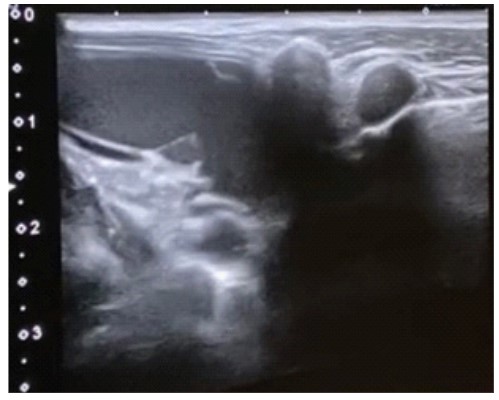
On further examination a compressible mass with visible pulsatility was observed. There was no palpable pulse, thrill, or audible bruit. The mass exhibited engorgement while speaking or other Valsalva maneuvers. A cervical vascular ultrasound demonstrated fusiform dilation of the internal jugular vein with no luminal thrombus, compressible throughout the neck extension (Figure 2). Normal contralateral exam. Transthoracic echocardiography, performed to exclude associated venous anoma- lies, was unremarkable.
Discussion
Jugular vein phlebectasia is a rare congenital anomaly characterized by isolated fusiform dilation of a venous segment [1]. It can alternatively occur after iatrogenic actions, as vascular catheterization or neck surgery, or trauma, inflammation or degenerative disease [3]. It is often asymptomatic and discovered incidentally but warrants differentiation from other cervical masses, such as laryngoceles, lymphatic malformations, hemangioma or superior mediastinal tumors (e.g., cystic hygromas) [1,2]. Imaging studies, particularly ultrasonography, are essential for accurate diagnosis and treatment decision [3].
Conservative approach is the norm, leaving surgical intervention for symptomatic cases or those with significant cosmetic or psychological concerns [3]. Misdiagnosis can lead to unnecessary invasive investigations or treatments, emphasizing the need for awareness of this benign condition among clinicians.
This case underscores the importance of recognizing jugular vein ectasia as a rare but benign entity. Prompt identification through clinical evaluation and imaging can prevent misdiagnosis and reassure caregivers of its non-threatening nature.

References
- Raffaele A, Gazzaneo M, Romano P, Gorone MSP, Avolio L. Congenital Internal Jugular Phlebectasia: An Anomaly Still Poorly Recognized. European J Pediatr Surg Rep. 2023; 11: e40–e43.
- Figueroa-Sanchez JA, Ferrigno AS, Benvenutti-Regato M, CaroOsorio E, Martinez HR. Internal jugular phlebectasia: a systematic review. Surg Neurol Int. 2019; 10: 106.
- Alkusayer MM, Alharbi AS, Aljabri NM, Saqer RMA, Alhammad BN, Alahmadi RM. (n.d.). Internal jugular vein phlebectasia: A systematic review of therapeutic approaches in Pediatrics. International Journal of Pediatric Otorhinolaryngology. 2023; 175: 111720.