
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Incidental finding during EBUS-TBNA
Sofia Martins De Castro1*; Paulo Matos2; Luís Vaz Rodrigues2; Michele De Santis2; Lourdes Barradas2
1Department of Pulmonology, Local Health Unit of the Aveiro Region, Portugal.
2Department of Pulmonology, Portuguese Institute of Oncology of Coimbra Francisco Gentil, Portugal.
*Corresponding Author : Sofia Martins De Castro
Department of Pulmonology, Local Health Unit of
the Aveiro Region, Portugal.
Tel: +35-1914500054;
Email: sofiafcastro@hotmail.com
Received : Jan 28, 2025
Accepted : Feb 13, 2025
Published : Feb 20, 2025
Archived : www.jcimcr.org
Copyright : © De Castro SM (2025).
Citation: De Castro SM, Matos P, Rodrigues LV, De Santis M, Barradas L. Incidental finding during EBUS-TBNA. J Clin Images Med Case Rep. 2025; 6(2): 3476.
Description
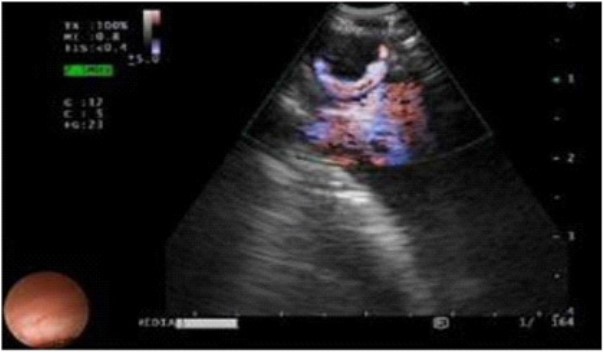
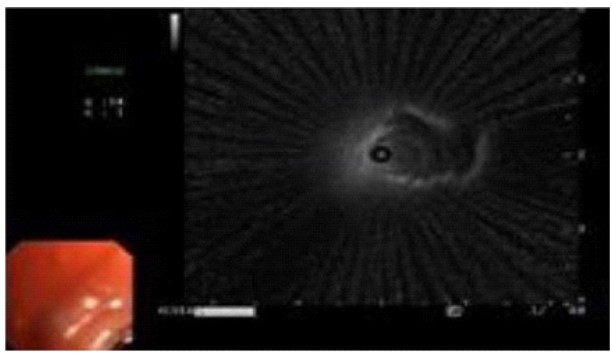
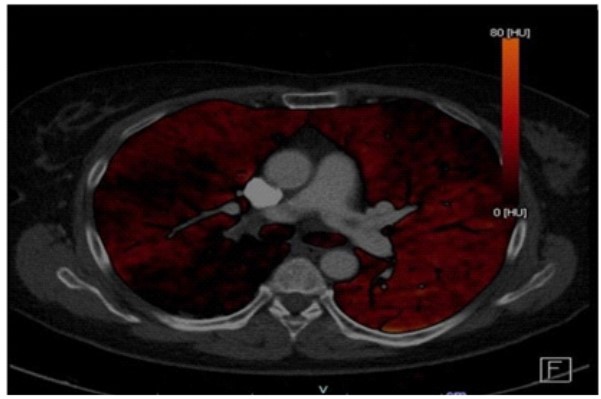
Patients with malignancies, particularly advanced-stage cancers, are at an increased risk for thromboembolic events, such as Pulmonary Embolism (PE). Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) is indispensable for the diagnosis and staging of thoracic malignancies and evaluating metastatic extra-thoracic tumors. Additionally, EBUS offers insights into vascular pathologies, including PE, through systematic mediastinal assessment [1,2]. We present the case of a 58-year-old woman diagnosed with uterine sarcoma, referred for EBUS-TBNA to investigate suspected pulmonary and mediastinal metastasis noted on PET-CT. During the ultrasound examination of the hilar area, an enlarged 10R lymph node was sampled, and a hypoechoic structure within the right pulmonary artery branch was identified (Figure 1), suggestive of a PE. Complementary inspection with radial EBUS in RB10 revealed of a small, eccentric, lobulated echogenic lesion in the proximal position (Figure 2). Subsequent contrast-enhanced chest CT and iodine mapping confirmed thrombi in the right upper and lower lobar pulmonary arteries, extending into approximately 10% of the left pulmonary artery (Figures 3 & 4). Similar to previously reported findings, EBUS enabled the identification of a potentially life-threatening thromboembolic event, underscoring its role beyond traditional cancer staging [3,4]. This case highlights the extended diagnostic potential of EBUS-TBNA beyond conventional oncological staging. While the procedure was primarily conducted to evaluate metastatic spread, it incidentally revealed a critical thromboembolic event. This underscores the value of thorough mediastinal and hilar evaluation during EBUS, which can uncover clinically significant findings. Broadening the application of EBUS in oncological care may enhance patient management by detecting unexpected pathologies [1,3].

References
- Endobronchial Ultrasound for the Screening of Pulmonary Embolism Respirology. 2023; 102: 601-607.
- Fantin A, Castaldo N, Ielpo A, et al. Pulmonary Embolism as a Finding During Endobronchial Ultrasound. Respir Med Case Rep. 2021; 34: 101491.
- Pulmonary Embolism Diagnosed During Endobronchial Ultrasound. Arch Bronconeumol. 2013; 49: 305-306.
- Herth FJ, Ernst A, Becker HD. Diagnosis of Pulmonary Thromboembolism with Endobronchial Ultrasound. Eur Respir J. 2008; 32: 1416-1417.