
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Ovarian cancer in umbilical hernia – Case report
Katarzyna Kwas*; Agnieszka Wilamowska; Maria Szubert; Jacek R Wilczyński
Department of Surgical and Oncologic Gynaecology, 1st Department of Gynaecology and Obstetrics, Medical University of Lodz, Poland.
*Corresponding Author : Katarzyna Kwas
Department of Surgical and Oncologic Gynaecology,
1st Department of Gynaecology and Obstetrics,
Medical University of Lodz, Poland.
Email: katarzyna.kwas@stud.umed.lodz.pl
Received : Jan 27, 2025
Accepted : Feb 14, 2025
Published : Feb 21, 2025
Archived : www.jcimcr.org
Copyright : © Kwas K (2025).
Abstract
Background: Ovarian cancer is currently the fifth leading cause of cancer-related deaths among women worldwide. It is an aggressive disease that is frequently detected at advanced stages. Patients often present with nonspecific pelvic or abdominal symptoms. Initial diagnostic tests include transvaginal ultrasonography and serum Cancer Antigen 125 (CA-125) measurement.
Case study: A 75-year-old female patient with asthma, chronic kidney disease, and hypertension presented with abdominal pain and defecation disorders and was admitted to the department. Ultrasonography demonstrated abnormalities in the uterus and both pelvic and abdominal cavities. Computed tomography determined pathological tissue masses around the umbilicus in contact with the transverse colon, small intestine, and uterus. Polycyclic structure with numerous uterine calcifications and enlarged inguinal nodules were described. The patient was qualified for the surgery because of subileus symptoms. The procedure was primarily palliative due to the beginning of intestinal transit disorders. The histopathological studies confirmed ovarian endometrioid adenocarcinoma G2 with infiltration on the anterior wall of the omental sac, greater omentum, peritoneum, uterus, and uterine myoma. The patient was not treated with platin-based chemotherapy due to lack of consent.
Conclusion: Ovarian cancer is an aggressive disease often diagnosed in advanced stages. Metastasis to the umbilical hernia region is rare and imposes differentiation with gastrointestinal tumors. Fast surgical intervention is usually required in such cases due to the high risk of bowel obstruction in the metastatic hernia region and preferred to neoadjuvant therapy.
Citation: Kwas K, Wilamowska A, Szubert M, Wilczynski JR. Ovarian cancer in umbilical hernia – Case report. J Clin Images Med Case Rep. 2025; 6(2): 3478.
Background
Ovarian cancer is one of the most common cancers among women worldwide and a leading cause of gynecologic cancer-related deaths. Despite significant advances in diagnostic and therapeutic strategies, the prognosis for ovarian cancer remains poor due to its often-asymptomatic nature in early stages, leading to delayed diagnosis. The disease encompasses a heterogeneous group of malignancies arising from the epithelial, stromal, or germ cells of the ovary, with epithelial ovarian cancer accounting for approximately 90% of cases. Risk factors for ovarian cancer include advanced age, family history, BRCA1 and BRCA2 mutations, and conditions like endometriosis. Protective factors, such as oral contraceptive use and multiparity, are associated with hormonal influences on ovarian physiology. The disease typically presents in women over 50 years of age, though it can occur in younger patients, particularly in those with a ge- netic predisposition [1,2]. Symptoms of ovarian cancer, often vague and non-specific, may include abdominal bloating, pelvic pain, early satiety, and urinary urgency, contributing to delayed recognition. Current diagnostic modalities include transvaginal ultrasound, serum tumor markers like CA-125, and advanced imaging techniques, but no reliable screening test exists for early detection in the general population [3]. The management of ovarian cancer relies on a combination of cytoreductive surgery and platinum-based chemotherapy, with recent advances in targeted therapies, including PARP inhibitors, offering improved outcomes for specific subsets of patients. However, recurrence rates remain high, necessitating ongoing research to improve early detection, prognostic assessment, and treatment options.
This case report highlights a unique presentation of ovarian cancer, underscoring the challenges in diagnosis and the importance of personalized therapeutic approaches. By exploring this case, we aim to contribute to understanding the disease’s clinical spectrum and advance discussions on optimizing patient care, especially when presenting with a disease requiring immediate intensive treatment.
Case study
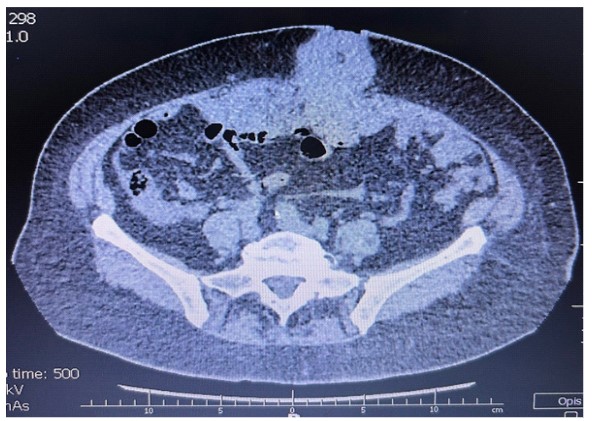
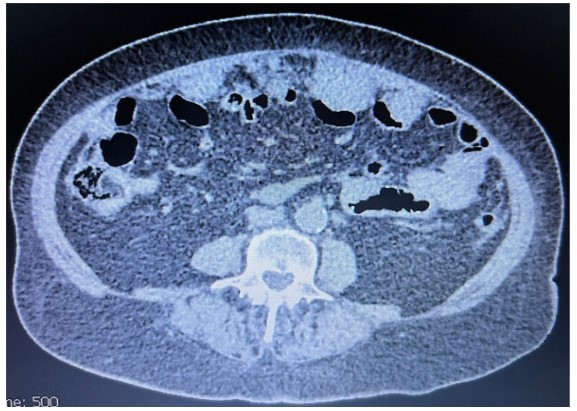
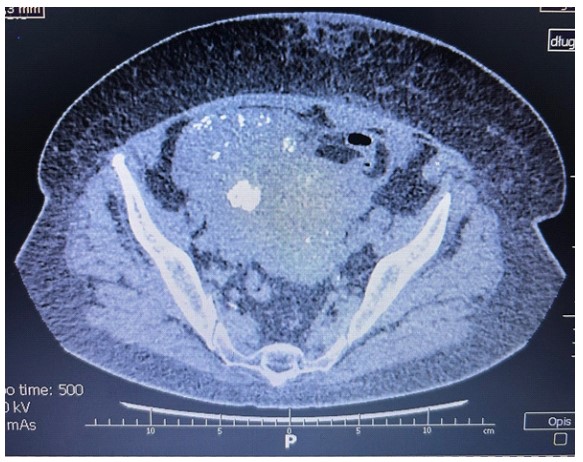
A 75-year-old female patient with asthma, chronic kidney disease, and hypertension. The patient had a history of 2 pregnancies and 2 childbirths and no data regarding the family history. The female presented with abdominal pain and defecation disorders and was admitted to the clinic. The laboratory results showed multiple abnormalities, including hemoglobin 11, 6 g/ dl (n: 11, 5-15, 5 g/dl), creatinine 1, 54 mg/dl (n: 0, 5-0, 9 mg/ dl), TSH 6, 36 ulU/ml (n: 0, 270-4, 200 ulU/ml), and the tumor marker CA-125 179, 2 u/ml (n: <35 U/ml). Physical examination revealed a 7-8 cm hernia in the umbilicus area. Ultrasonography demonstrated bulky mass of the uterus and homoechogenic nodules. Computed tomography determined pathological tissue masses measuring 83×60×70 mm around the umbilicus, which were in contact with the transverse colon, small intestine, and uterus, suggesting peritoneal grafts. Polycyclic structure with numerous calcifications measuring 131×100×82 mm in the uterus and enlarged inguinal lymph nodes measuring 9×18 mm were described.
Moreover, at the outer edge of the liver, thin layer of the fluid was up to 10 mm, and at the outer edge of the spleen, up to 12 mm. A subcapsular, hypodense focus of 11 mm in liver segment II was determined as too small for unequivocal assessment. The pancreas and spleen were not enlarged, homogeneous, and without perceptible focal changes that were distinguishable in the native phase.
The patient was qualified for the surgery. Longitudinal median laparotomy, radical removal of the uterus with adnexa, pelvic peritonectomy and left colic gutter, total omentectomy, rectal shaving, and excision of the tumor from the umbilical region and umbilical hernia repair were performed. Minor nodules on the small intestine, carcinomatosis on the diaphragm, and infiltration of 3-4 epiploic appendices through the intestine wall were left. The procedure was primarily palliative due to the subileus and the urgent need to restore intestinal passage. The histopathological studies showed the presence of ovarian endometrioid adenocarcinoma G2 with infiltration on the anterior wall of the omental sac, greater omentum, peritoneum, uterus, and uterine myoma. Immunohistochemistry defined CKAE1/AE3 (+), CK7 (+/-), vimentin (+), napsin (-), CDX2 (-), CK20 (+), ER(-/+), PR(-), ki67(+), p16(+/-), p53 (-), WT1(-), PAX8(-/+). There were lymph nodes (of greater omentum) without metastases. FIGO grade was assessed as IV.
After the surgery, the patient was referred for platin-based chemotherapy; however, the patient did not consent due to personal reasons. According to the patient’s family, the patient was satisfied with her life and attended several family events after the surgery. However, six months later, the patient was admitted to the neurological ward due to a cerebral stroke. As her daughter stated, multiple metastases in the lungs and liver were found in CT. The patient died during the hospitalization. Data regarding the patient’s last hospital stay wasn’t obtained.
Discussion
Ovarian cancer presenting in an umbilical hernia is an exceedingly rare phenomenon, underscoring the importance of clinical vigilance in evaluating atypical hernia contents. The umbilicus is a recognized site for metastasis in ovarian cancer, known as Sister Mary Joseph’s nodule, and its incidence ranges from 1% to 3% [4,5]. However, primary ovarian tumors manifesting within an umbilical hernia sac are scarcely documented. Millar et al. reported in their work six patients with ovarian cancer in reducible umbilical hernia, two of the described cases were patients with ovarian adenocarcinoma [6]. Karabulut et al. described an incarcerated umbilical hernia with a granulosa cell tumor of the ovary, whereas Liu et al. discussed an ovarian adenocarcinoma with metastasis to the umbilicus [7,8]. All these reports show that the management of ovarian cancer within an umbilical hernia necessitates a multidisciplinary approach. Surgical intervention often involves resection of the hernia sac with oncological clearance, followed by appropriate adjuvant therapy based on staging and histology.
The clinical implications of this finding are significant. Hernias containing neoplastic tissue are often mistaken for simple reducible or incarcerated hernias, potentially delaying diagnosis. Imaging modalities such as CT and Magnetic Resonance Imaging (MRI) play a pivotal role in identifying abnormal adnexal structures and ruling out concurrent malignancies. Histopathological examination remains the gold standard for confirming the diagnosis and determining the histological subtype, which is critical for tailoring therapeutic strategies.
This case emphasizes the need for heightened awareness among surgeons and oncologists regarding atypical presentations of ovarian cancer, as early recognition and intervention can significantly impact prognosis. Furthermore, reporting such rare cases contributes to the growing body of literature, guiding future diagnostic and therapeutic frameworks.
Conclusion
Ovarian cancer is an aggressive disease that, in some cases, may be initially impossible to remove in its whole range. Metastasis to the umbilical hernia region is rare and imposes differentiation with gastrointestinal tumors. Fast surgical intervention is usually required in such cases due to the high risk of bowel obstruction in the metastatic hernia region.
References
- Chandra A, Pius C, Nabeel M, Nair M, Vishwanatha JK, Ahmad S, et al. Ovarian cancer: Current status and strategies for improving therapeutic outcomes. Cancer Med. 2019; 8: 7018-7031.
- Tanha K, Mottaghi A, Nojomi M, Moradi M, Rajabzadeh R, Lotfi S, et al. Investigation on factors associated with ovarian cancer: an umbrella review of systematic review and meta- analyses. J Ovarian Res. 2021; 14: 153.
- Zhang R, Siu MKY, Ngan HYS, Chan KKL. Molecular Biomarkers for the Early Detection of Ovarian Cancer. Int J Mol Sci. 2022; 23: 12041.
- Kouira M, Bannour I, Ben Abdesslem MR, Abdessayed N, Bannour B. Ovarian Cancer Was Discovered in Sister Mary Joseph’s Nodule. Case Rep Med. 2022; 2022: 5131705.
- Piura B, Meirovitz M, Bayme M, et al. Sister Mary Joseph’s nodule originating from endometrial carcinoma incidentally detected during surgery for an umbilical hernia: a case report. Arch Gynecol Obstet. 2006; 274: 385-388.
- Millar RC, Geelhoed GW, Ketcham AS. Ovarian cancer presenting as umbilical hernia. J Surg Oncol. 1975; 7: 493-6.
- Karabulut Z, Aydin O, Onur E, Celik NY, Moray G. Giant ovarian tumor presenting as an incarcerated umbilical hernia: a case report. J Korean Med Sci. 2009; 24: 539-41.
- Liu R, Luo S, Yang X, Wang G, Lu B, et al. Ovarian cancer with umbilical metastasis: A case report and literature review. J Clin Images Med Case Rep. 2024; 5: 3054.