
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 6
Polymicrobial empyema: Description of clinical cases in children
Mendez Ana Paula1; Alonso Emilia1; Badia Federica1; Mota Inés2; Pirez María Catalina2*
1Pediatric Academic Unit A, Pediatric Infectology, Faculty of Medicine, University of the Republic, Montevideo, Uruguay.
2Microbiology Laboratory of the Pereira Rossell Hospital Center (CHPR), Montevideo, Uruguay.
*Corresponding Author : Pirez Maria Catalina
Pediatric Academic Unit A, Pediatric Infectology,
Faculty of Medicine, University of the Republic,
Montevideo, Uruguay.
Email: mcpirez@yahoo.com
Received : Jan 24, 2025
Accepted : Feb 14, 2025
Published : Feb 21, 2025
Archived : www.jcimcr.org
Copyright : © Catalina PM (2025).
Abstract
Pleural infection is a severe and complex disease with significant morbidity and mortality worldwide, affecting both children and adults. Polymicrobial etiology is considered very rare in children and adolescents, and most cases are described in adults. We describe two cases of polymicrobial empyema the first one a 6 years old boy with congenital pulmonary airway malformation type I in the right lung and the second one an adolescent 13 years old with multiple dental septic foci and periodontitis. Bacteriological Gram stain and culture demonstrate polymicrobial isolates. Medical and surgical treatment resolved the infection.
Citation: Paula MA, Emilia A, Federica B, Ines M, Catalina PM. Polymicrobial empyema: Description of clinical cases in children. J Clin Images Med Case Rep. 2025; 6(2): 3479.
Background
Pleural infection is a severe and complex disease with significant morbidity and mortality worldwide, affecting both children and adults [1-3]. Long hospital admissions and the need for invasive treatments, contribute to the high healthcare costs associated with this disease [2,3]. Usually, Pleural Empyema (PE) has a monomicrobial cause, where Streptococcus pneumoniae remains the most common etiology in the pediatric population, followed by H. influenzae, S. aureus and S. pyogenes [3-5].
Polymicrobial etiology is considered very rare in children and adolescents, and most cases are described in adults [6]. Polymicrobial etiology is typically linked to oral flora pathogens and is especially associated with individuals with neurological or immune disorders and adults with conditions such as alcoholism or kidney disease.
This article reports two clinical cases of PE, with polymicrobial etiology, in previously healthy pediatric patients. We describe microbiological diagnosis and workup to identify an underlying condition.
Case report
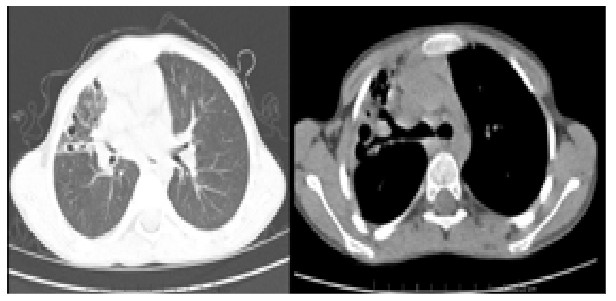
Case 1: A 6-year-old male, previously healthy with up-to-date vaccinations, that lives in adverse environment conditions. He had a history of two previous episodes of right-sided Community Acquired Pneumonia (CAP), improving clinically but with unresolved radiological findings (Figure 1). Tuberculosis infection was ruled out. He presented with respiratory symptoms and fever. Physical examination showed signs of pleural involvement on the right side. Chest X-ray revealed right-sided pneumonia with pleural effusion. Pleural fluid analysis revealed in Gram stain, numerous gram-negative bacilli and a few Gram-positive and Gram-negative diplococci; the culture indicated the presence of polymicrobial isolates. Treatment included pleural drainage for 20 days, 21 days of intravenous antibiotics, including ceftriaxone, clindamycin, gentamicin, and metronidazole, followed by 28 days of oral antibiotics, amoxicillin - clavulanic acid. Despite no radiological improvement, a CT scan revealed cystic lesions in the right lung (Figures 2 and 3). Surgical lobectomy of the right upper lobe was performed, with pathology indicating congenital pulmonary airway malformation type I.
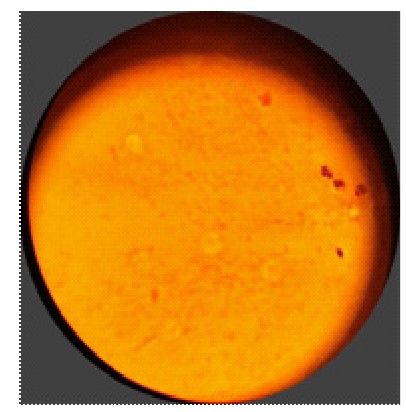
Case 2: A 13-year-old female with no chronic illnesses or toxic habits and up-to-date vaccinations, that lives in adverse environmental conditions, presents with right abdominal pain and fatigue. Physical examination showed peritoneal irritation signs. An exploratory laparoscopy revealed no abnormalities. She later developed right-sided pleural involvement, and chest X-ray showed pleural effusion (Figure 4). Pleural fluid analysis confirmed empyema, Gram stain is described in (Figure 5), and culture indicates the presence of polymicrobial isolates. The patient underwent thoracic drainage for 36 days. Despite persistent fever, imaging follow-up revealed an abscess in the right upper lobe. She received antibiotics, ampicillin sulbactam and clindamycin, for six weeks and surgical abscess drainage. Streptococcus constellatus was identified from the abscess specimen, by Mass Spectrometry, by Matrix-Assisted Laser Desorption/ Ionization Time-of-Flight (MALDI TOF). Orthodontia evaluation was performed, with multiple dental septic foci and periodontitis was observed, removing 2 dental pieces was necessary.



Discussion
Polymicrobial etiology of PE in children, particularly involving oral aerobic and anaerobic microorganisms, is rare. In literature research we only find a case report of 3 pediatric patients, 2 of them with neurologic disabilities, in which polymicrobial etiology of PE was identified [7]. Most of the bacteria isolets in pleural samples correspond to oral cavity and dental microbiome [7].
In adults there seems to be an increase in polymicrobial and monomicrobial not streptococcus cases of pleural infection [8,9]. Anaerobes exhibited the highest mean abundance, followed by other Gram-negative bacteria, and bacteria of the S anginosus group [8,9].
The most common comorbidities associated with PE in adults were dental disease, followed by heart disease and diabetes mellitus, neurological disabilities, and less frequent but with major mortality liver disease and malignancy [10].
Both of our patients, although coming from adverse social and economic environments, didn´t report previous chronic conditions. Case 2, beside poor oral hygiene, periodontitis and septic focus, that recurred dental treatment involving the extraction of teeth, were identified as infectious sources.
In Case 1 a pulmonary congenital malformation was identified. Congenital Cystic Adenomatoid Malformation, the most common malformation in children, presents clinically as respiratory infections or recurrent pneumonia [11]. There are no reports that polymicrobial PE are more common in this group of patients.
Conclusion
Physiological micro aspiration in patients with periodontal disease, combined with local or regional conditions, can lead to pleuropulmonary complications.
This work aims to raise awareness about this etiology and its predisposing factors.
References
- Lisboa T, Waterer GW, Lee YC. Pleural infection: changing bacteriology and its implications. Respirology. 2011; 16: 598e603.
- Grijalva CG, Zhu Y, Nuorti JP, Griffin MR. Emergence of parapneumonic empyema in the USA. Thorax. 2011; 66: 663e8.
- Buonsenso D, Cusenza F, Passadore L, Bonanno F, Calanca C, Mariani F, et al. Parapneumonic empyema in children: a scoping review of the literature. Ital J Pediatr. 2024; 50: 136.
- Alban Le Monnier, Etienne Carbonnelle, Jean-Ralph Zahar, Muriel Le Bourgeois, Eric Abachin, Gilles Quesne, et al. Microbiological Diagnosis of Empyema in Children: Comparative Evalua- tions by Culture, Polymerase Chain Reaction, and Pneumococcal Antigen Detection in Pleural Fluids. Clinical Infectious Diseases. 2006; 42: 1135–1140.
- Pírez MC, Algorta G, Chamorro F, Romero C, Varela A, Cedres A, et al. Changes in hospitalizations for pneumonia after universal vaccination with pneumococcal conjugate vaccines 7/13 valent and haemophilus influenzae type b conjugate vaccine in a Pediatric Referral Hospital in Uruguay. Pediatr Infect Dis J. 2014; 33: 753-9.
- Yamazaki A, Ito A, Ishida T, Washio Y. Polymicrobial etiology as a prognostic factor for empyema in addition to the renal, age, purulence, infection source, and dietary factors score. Respir Investig. 2019; 57: 574-581.
- Ploton MC, et al. Likely false-positive pneumococcal antigen test BinaxNOW due to Parvimonas micra. CHEST. 2018; 153: e71-e77.
- Kanellakis NI, Wrightson JM, Gerry S, Ilott N, Corcoran JP, Bedawi EO, et al. The bacteriology of pleural infection (TORPIDS): an exploratory metagenomics analysis through next generation sequencing. Lancet. 2022; 3: e294-302.
- Chan KPF, Ma TF, Sridhar S, Lam DCL, Ip MSM, Ho PL. Changes in Etiology and Clinical Outcomes of Pleural empyema during the COVID-19 Pandemic. Microorganisms. 2023; 11: 303.
- Yamazaki A, Ito A, Ishida T, Washio Y. Polymicrobial etiology as a prognostic factor for empyema in addition to the renal, age, purulence, infection source, and dietary factors score. Respir Investig. 2019; 57: 574-581.
- Jhun BW, Kim SJ, Kim K, Kim S, Lee JE. The Clinical Courses of Patients with Congenital Cystic Adenomatoid Malformation Complicated by Pneumonia. Yonsei Med J. 2015; 56: 968-75.