
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A rare case of visceral leishmaniasis presenting as alithiasic cholecystitis: Case report
M Nacir1,2*; M Lagrine2; R El Qadiry1; H Nassih1; A Bourahouat1; R Moutaj2; I Ait Sab1
1Department of Pediatrics B, CHU Mohammed VI, Marrakech, Morocco.
2Department of Parasitology and Mycology, Avicenne Military Hospital, CHU Mohammed VI, Morocco.
*Corresponding Author : Maroua Nacir
Department of Pediatrics B, CHU Mohammed VI,
Marrakech, Morocco.
Email: marouaanac@gmail.com
Received : Jan 27, 2025
Accepted : Feb 18, 2025
Published : Feb 25, 2025
Archived : www.jcimcr.org
Copyright : © Nacir M (2025).
Abstract
Fever, splenomegaly, and pancytopenia are common signs of Visceral Leishmaniasis (VL), an uncommon but dangerous parasite infection. Rare appearances, however, may make diagnosis difficult. Here, we describe a case of a 1-year-old boy from Beni Mellal, Morocco, who had intermittent fever, jaundice, and stomach ache for a month. Laboratory results showed anemia, lymphocytosis, and increased liver enzymes, whereas clinical evaluation revealed jaundice without enlargement of the liver or spleen. Acalculous cholecystitis was indicated by abdominal ultrasonography results, which showed a thicker gallbladder wall without biliary duct dilatation or hepatomegaly. A bone marrow biopsy revealed Leishmania amastigotes, which were subsequently verified by serology.
Jaundice resolved after 28 days of treatment with meglumine antimoniate (Glucantime), which also produced notable improvements in the laboratory and clinical settings.
This case highlights the necessity of including VL in the differential diagnosis of febrile jaundice in endemic locations is, which demonstrates an unusual form of VL presentation.
In order to prevent problems and guarantee positive patient outcomes, early diagnosis and treatment are crucial.
Keywords: Visceral leishmaniasis; Acalculous cholecystitis; Febrile jaundice; Hepatosplenomegaly; Tropical diseases; Rare pediatric infections.
Citation: Nacir M, Lagrine M, Qadiry RE, Nassih H, Bourahouat A, et al. A rare case of visceral leishmaniasis presenting as alithiasic cholecystitis: Case report. J Clin Images Med Case Rep. 2025; 6(2): 3482.
Introduction
Visceral Leishmaniasis (VL) is a systemic infection and a type of leishmaniasis disease caused by the parasitic infection of Leishmania species and is primarily spread by the bite of infected sandflies. It is known to be endemic in certain regions of the world and among certain group of people, particularly children and those with immunocompromised status. VL is commonly presented with prolonged fever, considerable weight loss, hepatosplenomegaly with associated pancytopenia, which can be suspected clinically without much difficulty in endemic areas.
Although jaundice can be seen as an impact when liver involvement or hemolysis exists, it is not common for patients with VL, to have jaundice and symptoms of biliary tract involvement to be prominent. Alithiasic cholecystitis, or the inflammation of the gall bladder in absence of the gallstones, is even rarer in association with VL. With such atypical presentations, correct diagnosis can be deferred, which will result in delay in treatment, and can lead to the worsening of the prognosis of the patients.
This case report describes a 2-year-old child with VL presenting as jaundice and alithiasic cholecystitis, an uncommon initial presentation. By documenting this rare presentation, we intend to make other clinicians aware that the presence of similar symptoms among children from endemic regions should suggest the possible inclusion of VL in the differential diagnosis.
Case presentation
A 1-year-8-month-old male child from Beni Mellal - Morocco, presented with complaints of prolonged fever (up to 38.5°C) lasting one month, accompanied by jaundice. The jaundice was characterized by dark-colored urine and pale stools, suggestive of a cholestatic pattern. These symptoms were associated with general deterioration, including fatigue and poor appetite. His medical history was unremarkable, with no known chronic liver disease, toxic exposures, medication use, or similar cases within the family. His vaccinations were up-to-date according to the national immunization schedule, and his psychomotor development was appropriate for age.
On admission, the child appeared visibly jaundiced with scleral icterus. General physical examination was otherwise normal, with weight at 10 kg and height of 84 cm, which was average for his age. Abdominal examination revealed a distended abdomen with shifting dullness, indicating possible ascites. There was no hepatomegaly, splenomegaly, or palpable masses, and no clinical signs of chronic liver disease. The remainder of the examination showed no abnormalities.
Laboratory investigations on admission showed anemia with a hemoglobin level of 7.8 g/dL, microcytic hypochromic indices (MCV: 66 fL, MCH: 20 pg), leukopenia with a total leukocyte count of 6960/mm³ (including neutrophils 1385/mm³ and lymphocytes 4329/mm³), and thrombocytopenia with platelets at 96,000/mm³. Ferritin levels were elevated at 277 ng/mL. Liver function tests revealed marked elevations in transaminases (AST: 971 IU/L, 24 times the normal upper limit, ALT: 293 IU/L 7×N) and total bilirubin at 81 mg/L, with indirect bilirubin at 58.5 mg/L and direct bilirubin at 29 mg/L. Gamma-Glutamyl Transferase (GGT) was elevated at 3 times the normal upper limit, while the prothrombin time was decreased at 65% and albumin was low at 27 g/L.
Serological testing for viral hepatitis and other common infectious agents was negative.
These findings are consistent with a cholestatic pattern of jaundice, suggesting hepatobiliary involvement.
An abdominal ultrasound was performed to investigate potential causes of febrile jaundice with abdominal pain and to rule out surgical pathology. The ultrasound revealed a mild amount of free fluid in the abdomen and a gallbladder with a thickened, layered wall measuring approximately 4 mm. No intra- or extrahepatic biliary dilation was observed, consistent with alithiasic cholecystitis. The liver was of normal size with a homogeneous structure, and the spleen appeared normal.
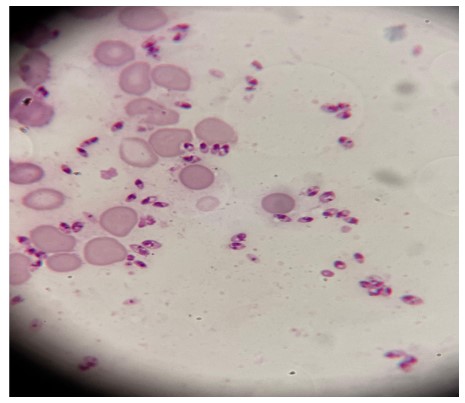
In light of the pancytopenia and the systemic signs, further diagnostic evaluation was undertaken. Bone marrow aspiration revealed Leishmania bodies, confirming a diagnosis of visceral leishmaniasis. Serology for Leishmania by ELISA was positive for both IgG and IgM, with a quantitative result of 31 NTU, corroborating the diagnosis.
The patient was started on Meglumine antimoniate at a dose of 60 mg/kg/day for 28 consecutive days. During the treatment period, a weekly follow-up ultrasound was performed, which showed progressive improvement. Liver function tests and other clinical parameters were monitored closely, with normalization achieved by the end of the treatment course. Over the treatment period, the jaundice and abdominal pain progressively improved, along with a return to baseline energy levels and appetite. Repeat laboratory evaluations showed improvements in liver function tests, blood counts, and overall clinical status. The child was discharged in stable condition with follow-up planned to monitor for any potential recurrence or lingering effects.
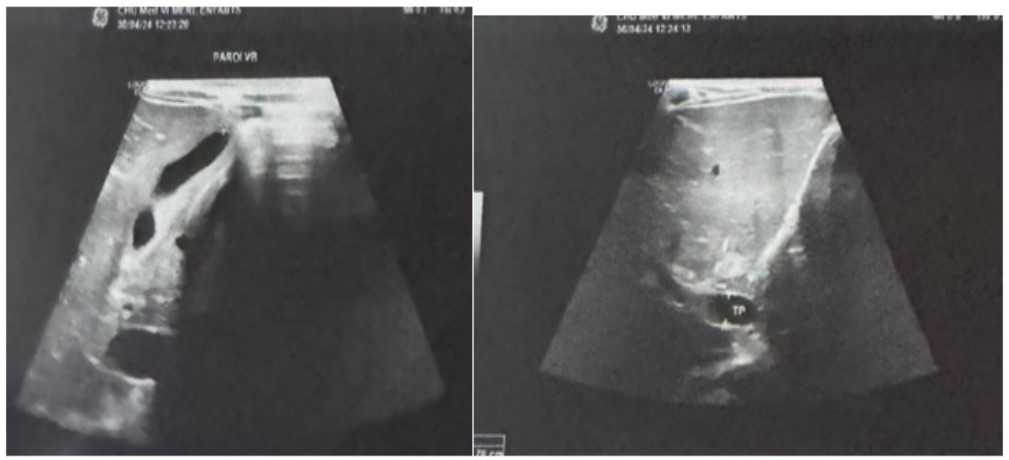
Table 1: Laboratory profile evolution pre- and post-treatment in our case.
| Parameter | Initial value | Post-treatment value |
|---|---|---|
| Hemoglobin | 7.8 g/dL | 10.5 g/dL |
| MCV | 66 fL | 78 fL |
| MCH | 20 pg | 26 pg |
| Leukocyte Count | 6,960 /mm³ | 8,500 /mm³ |
| Neutrophils | 1,385 /mm³ | 3,500 /mm³ |
| Lymphocytes | 4,329 /mm³ | 3,000 /mm³ |
| Platelets | 96,000 /mm³ | 250,000 /mm³ |
| Ferritin | 277 ng/mL | 120 ng/mL |
| AST | 971 IU/L | 45 IU/L |
| ALT | 293 IU/L | 35 IU/L |
| Total Bilirubin | 81 mg/L | 12 mg/L |
| Direct Bilirubin | 29 mg/L | 3 mg/L |
| Indirect Bilirubin | 58.5 mg/L | 9 mg/L |
| GGT | 140 IU/L | 30 IU/L |
| Prothrombin Time (PT) | 65% | 85% |
| Albumin | 27 g/L | 40 g/L |
Discussion
This case report describes an unusual presentation of Visceral Leishmaniasis (VL) in a young child with acalculous cholecystitis, an exceptionally rare manifestation of the disease. Typically, VL presents with prolonged fever, hepatosplenomegaly, pancytopenia, and weight loss. While gastrointestinal symptoms can occur, direct involvement of the gallbladder without gallstones (acalculous cholecystitis) is rarely documented in the literature. In this case, the initial symptoms of jaundice, abdominal pain, and fever posed diagnostic challenges and broadened the differential diagnosis, highlighting the complexities of diagnosing VL with atypical presentations.
The presence of acalculous cholecystitis in VL has been reported sporadically in cases documented by Cermeno et al. and Fahal et al. [4,5] indicating that although rare, this manifestation is possible and warrants clinical consideration, especially in endemic regions. Potential mechanisms include direct invasion of the Leishmania parasite into the gallbladder wall, immunemediated inflammation, or systemic inflammatory responses secondary to prolonged infection. Additionally, in VL, immunosuppression associated with systemic parasitic load may predispose to secondary bacterial infections or inflammation, which could contribute to gallbladder involvement.
Cermeno et al. [4] reported a case of acalculous cholecystitis in a patient with VL, highlighting the hepatobiliary pathology that can arise from leishmanial infection. In this case, there was no evidence of gallstones, and the ultrasound findings were similar to those observed in our patient, including thickened gallbladder walls without biliary dilatation, which is characteristic of acalculous cholecystitis.
In the case reported by Fahal et al. [5] leishmanial cholecystitis and colitis were found in a patient with VL, further supporting the notion that VL can involve multiple organs, including the gastrointestinal system. This case also emphasizes the need for careful evaluation of the hepatobiliary system in VL patients, especially when presenting with jaundice and abdominal pain, as the diagnosis may not always be straightforward.
The unusual presentation of VL with cholestatic jaundice was further discussed by Yadav et al. [6], who reviewed rare observations in VL. They note that although VL typically presents with hepatosplenomegaly, there are cases where jaundice may be the primary clinical manifestation, particularly in regions with high endemicity. The presence of fever, abdominal pain, and abnormal liver function tests in such cases, as seen in our patient, can mimic more common liver diseases, leading to misdiagnosis if VL is not considered early in the diagnostic workup.
In our case, the presence of pancytopenia and elevated liver enzymes raised suspicion for a systemic infection, and the subsequent identification of Leishmania amastigotes in bone marrow aspirates confirmed the diagnosis.
This process illustrates the need for a thorough diagnostic approach in endemic areas where VL may present atypically. Given the significant overlap in symptoms with other hepatobiliary diseases, VL should be part of the differential diagnosis in patients presenting with prolonged fever, hepatosplenomegaly, or pancytopenia, even when unusual symptoms like cholecystitis are present.
Regarding treatment, Meglumine antimoniate (Glucantime) was chosen due to its effectiveness and availability in North Africa, where it is commonly used to treat VL. Copeland and Aronson (2015) recommend a dose of 60 mg/kg/day for 28 days in pediatric VL cases, a protocol we followed in this case. Weekly monitoring of the patient’s liver enzymes, complete blood count, and abdominal ultrasound was conducted to ensure therapeutic efficacy and to detect any adverse effects. Antimonial compounds can cause side effects such as nephrotoxicity and pancreatitis, which underscores the importance of careful monitoring, especially in pediatric cases.
The patient’s response to treatment was favorable, with a gradual resolution of symptoms, normalization of liver function tests, and improvement in gallbladder inflammation on follow-up ultrasounds. This aligns with outcomes reported in the literature, where recovery with Meglumine antimoniate is generally favorable, though response rates and time to recovery can vary. Several studies have examined the effectiveness and recovery timeline with this drug. Sundar et al. demonstrated high efficacy with Meglumine antimoniate in treating VL in both children and adults, reporting that 80-90% of patients respond well to the standard 28-day treatment course. Additionally, Murray et al. [8] showed that while the majority of patients recover within a few weeks of therapy, the response rate may be slower in cases complicated by co-infections or atypical manifestations, such as those with visceral involvement like cholecystitis.
Table 2: Comparison of treatment, complications, and outcomes in visceral leishmaniasis cases with systemic involvement.
| Study | Treatment | Duration | Outcome | Organ involvement | Comments |
|---|---|---|---|---|---|
| Cermeno et al. [4] | Meglumine antimoniate | 28 days | Recovery | Hepatic involvement (cholecystitis) | No hepatic, splenic, or renal complications were observed. The patient responded well to the standard treatment regimen. |
| Fahal et al. [5] | Meglumine antimoniate | 28 days | Partial recovery | Liver, Colitis, cholecystitis | The patient developed leishmanial cholecystitis and colitis, which required extended monitoring, but the response was less favorable compared to isolated VL cases. |
| Yadav et al. [6] | Liposomal amphotericin B | 21 days | Recovery | Multi-organ failure | This case involved multi-organ failure, requiring a combination of therapies and intensive care, with a favorable recovery post-treatment. |
| Current Case | Meglumine antimoniate | 28 days | Full recovery | Hepatic involvement (cholecystitis) | The patient developed cholecystitis, a rare complication of VL, but responded well to the standard treatment of Meglumine antimoniate without any need for surgical intervention. Weekly follow-ups showed steady improvement. |
Furthermore, the effectiveness of Meglumine antimoniate was confirmed in various studies, where it was the first-line treatment in endemic areas. According to Sharma et al. [9] Meglumine antimoniate remains the gold standard treatment for pediatric VL, with a high cure rate of over 90%. However, they also noted that the treatment efficacy can be influenced by factors such as parasite strain, the patient’s immune status, and whether the infection has led to secondary complications like other organs involvement.
Pediatric VL cases present unique challenges, as children may have different pharmacokinetic profiles and increased susceptibility to drug toxicity. Requiring close attention to dosing adjustments and side-effect monitoring to balance efficacy and safety.
Conclusion
This case shows the clinician’s need to keep Visceral Leishmaniasis (VL) in the differential diagnosis of children febrile with jaundice and abdominal pain, even though the clinical picture is not classical as in this patient.
Although rare, VL does have atypical features including hepatic involvement and hence early diagnosis and treatment may have great impact on the outcomes.
In regions endemic to VL, such as Morocco, clinicians should maintain a high index of suspicion for VL, particularly in patients with persistent fever and signs of systemic involvement. The use of Meglumine antimoniate remains the cornerstone of treatment for pediatric VL, demonstrating efficacy in both uncomplicated and complicated cases, though monitoring for potential side effects is essential. Early initiation of therapy, combined with careful follow-up and monitoring, can lead to favorable clinical outcomes, as demonstrated in this case.
This case adds to the knowledge that there may be many different manifestations of VL and hence calls for more work to be done in the region including febrile children with abdominal signs in endemic countries. We recommend further studies on the mechanisms of other organ involvement in VL and the longterm sequelae in treated pediatric cases to improve the clinical management strategies.
References
- Ashford RW. The leishmaniasis as emerging diseases of the world. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2000; 94: 1-2.
- Jha A, Thakur R. Visceral leishmaniasis presenting as a cause of jaundice: A case report. The Pan African Medical Journal. 2017; 28: 45.
- Desjeux P. Leishmaniasis: Current situation and new perspectives. 2004.
- Cermeno JR, Caraballo AJ, Gonzalez J. Acalculous cholecystitis in a patient with visceral leishmaniasis. 2001.
- Fahal AH, El Hag IA, El Hassan AM, Hashim FA. Leishmanial cholecystitis and colitis in a patient with visceral leishmaniasis. 1995.
- Yadav P, Azam M, Ramesh V, Singh R. Unusual Observations in Leishmaniasis—An Overview. 2023.
- Sundar S, et al. Treatment of visceral leishmaniasis in children with meglumine antimoniate: clinical outcome and risk factors for treatment failure. The American Journal of Tropical Medicine and Hygiene. 2001; 65: 799-804.
- Murray HW, et al. Leishmaniasis: Diagnosis, Treatment and Monitoring. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2005; 99: 130-142.
- Sharma PM, et al. Efficacy of Meglumine antimoniate in the treatment of visceral leishmaniasis in Indian children. Journal of Infectious Diseases. 2003; 188: 947-953.
- Muller M, et al. Visceral leishmaniasis in children: treatment and follow-up in endemic regions. Journal of Pediatric Infectious Diseases. 2004; 23: 98-103.