
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Atypical presentation of prallethrin poisoning and its therapeutic challenges: Case report
Harsha Shahi1; Dhruv Jain1*; Trehan Prashant Singh2; Heena Shahi3; Shreya Jain4
1Junior Resident, Post Graduate Department of General Medicine, Subharti Medical College, India.
2Assistant Professor, Post Graduate Department of General Medicine, Subharti Medical College, India.
3Junior Resident, Department of Pathology, SS Institute of Medical Sciences, India.
4Intern, Lady Hardinge Medical College, India.
*Corresponding Author : Dhruv Jain
Junior Resident, Department of General Medicine,
Subharti Medical College, Meerut, India.
Tel: +91 8076513026
Email: jaindhruv256@gmail.com
Received : Jan 27, 2025
Accepted : Feb 18, 2025
Published : Feb 25, 2025
Archived : www.jcimcr.org
Copyright : © Jain D (2025).
Abstract
Acute human poisoning from pyrethroids, while infrequent, presents considerable diagnostic and therapeutic challenges. This case report highlights a rare instance of prallethrin poisoning, a pyrethroid derivative commonly found in mosquito repellents, and underscores the importance of early recognition and comprehensive management. A 24-year-old female was admitted with symptoms including breathlessness, chest pain, cough, and fever following the ingestion of a mosquito repellent containing prallethrin. On clinical examination, the patient exhibited signs of respiratory distress, pleural effusion, and neurological impairment. Diagnostic investigations, including chest radiography and bronchoscopy, confirmed pyrethroid toxicity as the underlying cause. The patient was promptly managed with intensive care support, including non-invasive ventilation, pleural effusion drainage, and symptomatic treatment to address respiratory and neurological symptoms. The patient showed substantial improvement with timely interventions and was discharged in stable condition. This case emphasizes the critical role of thorough history-taking, vigilant monitoring, and a multidisciplinary approach in managing pyrethroid toxicity. Despite its challenging presentation, the patient’s successful recovery illustrates the value of prompt and tailored therapeutic strategies in such rare poisoning cases.
Keywords: Pig tail; Pyrethroid insecticides; Pleural effusion; Non- invasive ventilation; Mosquito repellent toxicity.
Citation: Shahi H, Jain D, Singh TP, Shahi H, Jain S. Atypical presentation of prallethrin poisoning and its therapeutic challenges: Case report. J Clin Images Med Case Rep. 2025; 6(2): 3483.
Introduction
Pyrethroid compounds are extensively utilised as insecticides due to their broad range of applications and favourable toxicological properties, characterised by high selectivity and potency against insects while exhibiting relatively low toxicity in humans. The slow absorption of pyrethroids through the skin in humans, combined with their large body surface area and the quick breakdown into harmless substances, helps reduce their toxicity in humans [1].
Pyrethroids are classified into two distinct types based on their structural differences and corresponding clinical effects. Type I Pyrethroids: These compounds lack an α-cyano (alpha cyano) group in their chemical structure. Type II Pyrethroids: These contain a Cyano group (-CN) attached to the benzylic carbon atom. This structural addition enhances their insecticidal potency [2]. The presence of the cyano group in Type II pyrethroids contributes significantly to their increased toxicity and efficacy as insecticides [3].
Acute human poisoning from pyrethroids is rare, with the first documented case in 1982. Pyrethroids, derived from Chrysan- themum cinerarilifolium, are highly toxic to insects (2250 times more than mammals) due to increased sodium channel sensitivity, smaller body size, and lower body temperature [4]. Pyrethroid toxicity primarily affects excitable cells, such as nerve and muscle cells, by acting on sodium and chloride channels. Pyrethroids modify the gating of voltage-sensitive sodium channels, delaying their closure, which leads to prolonged sodium influx and repetitive firing, potentially causing conduction block and clinical symptoms like paraesthesia. Type II pyrethroids have a more prolonged effect and also act on voltage- dependent chloride channels, contributing to symptoms like salivation, myotonia, and seizures. At higher concentrations, pyrethroids may also affect GABA-gated chloride channels, which could explain the seizures in severe type II poisoning [5,6]. Commonly reported symptoms of pyrethroid exposure include facial paraesthesia, skin irritation (itching or burning), dizziness, nausea, vomiting, and in severe cases, muscle fasciculations. Based on animal studies of acute pyrethroid exposure, two distinct toxidromes have been identified. Type I pyrethroids cause reflex hyperexcitability and fine tremors, referred to as T syndrome or Type I syndrome. Type II pyrethroids are associated with incoordination, choreoathetosis, seizures, and effects on skeletal and cardiac muscle, as well as the salivary glands, collectively known as choreoathetosis- salivation or Type II syndrome [7].
Clinical manifestations are elusive, making differential diagnosis crucial, especially against organophosphate or organo-chlorine poisoning. Exposure history is key for accurate differ- entiation. Management involves mainly supportive care and symptomatic interventions, as there is no specific antidote. We present a rare case of a 24-year-old female who ingested prallethrin, resulting in the development of bilateral pleural effusion and acute lung injury. She was promptly managed and achieved a successful recovery, being discharged within two weeks of her initial presentation.
Case presentation
A 24-year-old female was brought to the Emergency Department with a chief complaint of breathlessness for 1 day, right- sided chest pain for 5 days, non-productive cough for 5 days, and intermittent fever for 5 days. She admitted to ingesting a mosquito repellent (All Out) containing prallethrin. Vital signs at admission were: BP 106/76 mmHg, PR 122/min, RR 20/min, SpO2 94% on room air, and temperature 98°F. A neurological exam showed she was conscious, oriented, with bilateral plantar flexion and normal-sized, reactive pupils. The cardiac exam revealed S1S2+ with no murmurs. The respiratory exam indicated bilateral air entry but with decreased breath sounds and bilateral crepitations. Electrocardiography revealed a normal sinus rhythm.
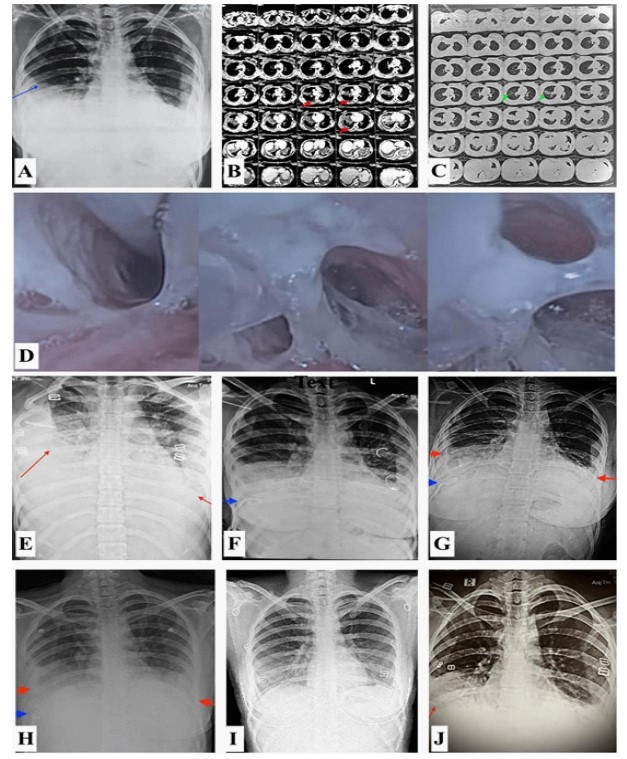
Routine blood investigations showed anemia (Hb - 6.3 mg/ dL), for which 2 PRBC units were transfused, and mildly deranged INR (1.48). All other blood investigations were within normal limits (Table 1). A chest X-ray revealed pleural effusion (Figure 1A), and a CECT chest (Figure 1B, C) showed ground glass opacity in the right middle lobe and basal segments of the left lower lobe, along with pleural fluid (1.7 cm and 9 mm strip thickness in the right and left pleural spaces, respectively). A Reverse Transcription Polymerase Chain Reaction (RT-PCR) test for COVID-19 was negative.
A diagnostic pleural tap indicated the pleural fluid to be exudative in nature (Table 1). Bronchoscopy revealed excessive secretions (Figure 1D), and a Bronchoalveolar Lavage (BAL) sample was sent for investigations, which later cultured positive for Candida albicans (Table 1). During the hospital stay, the patient’s condition worsened on day 3 (D3) with a fall in oxygen saturation and persistent shortness of breath. A follow-up X-ray revealed increased pleural effusion (right more than left) (Figure 1E), necessitating urgent intervention. A USG-guided pigtail catheter was inserted to address the pleural effusion. Initially on nasal prongs, she was shifted to a non-rebreather mask due to her worsening condition. When she failed to maintain adequate oxygenation via the non-rebreather mask, non-invasive ventilation was attempted. Due to the worsening clinical picture, the patient was transferred to the Intensive Care Unit (ICU). Bilevel Positive Airway Pressure (BiPAP) support was initiated for respiratory distress, and the pigtail catheter managed the pleural effusion. Intravenous atropine (0.6 mg every four hours) was administered for excessive secretions. The patient also received broad-spectrum IV antibiotics, antifungals as per culture sensitivity (Table 1), analgesics, antiemetics, proton-pump inhibitors, cough suppressants, corticosteroids, and regular nebulization as part of symptomatic treatment.
A chest X-ray was repeated after pigtail insertion (Figure 1F) to check the status of the pleural effusion and confirm the position of the catheter. On day 10 (D10), a chest X-ray (Figure 1G) showed resolving pleural effusion with underlying consolidation. On day 14 (D14), the output from the pigtail catheter was less than 25 mL over 48 hours. A repeat X-ray (Figure 1H) showed minimal effusion, and the pigtail catheter was subsequently removed. The patient’s clinical condition improved, as evidenced by a declining oxygen requirement and now on day 20 (D20) patient is maintaining saturation at 98% on nasal prongs at 2L O2/min subsequently to room air. A follow-up chest X-ray after three weeks (D21) (Figure 1I) showed resolved pleural effusion with underlying consolidation. The patient was scheduled for regular follow-up, and a chest X-ray taken two weeks later (Figure 1J) showed no signs of pleural effusion.
Discussion
This case of prallethrin poisoning underscores the complexities involved in diagnosing and managing acute pyrethroid toxicity, particularly given the infrequent occurrence of such cases in humans. Pyrethroids are generally regarded as safe due to their minimal absorption through human skin and rapid metabolism into inactive metabolites [5]. However, as demonstrated by this case, ingestion or significant exposure can lead to serious systemic toxicity, necessitating prompt and multidisciplinary medical intervention. The patient’s clinical presentation of respiratory distress, pleural effusion, and elevated inflammatory markers initially suggested a broad differential diagnosis, including infectious causes like COVID-19. The overlapping symptomatology of pyrethroid poisoning with other conditions can complicate the diagnostic process. However, the patient’s history of prallethrin ingestion, combined with findings of ground-glass opacities and pleural effusion on chest imaging, steered the diagnosis towards pyrethroid toxicity.
Table 1: Laboratory values across the treatment timeline.
| DAY 1 | D3 | D7 | D14 | D18 | D20 | D21 | |
|---|---|---|---|---|---|---|---|
| Hemoglobin | 6.3 | 8.2 | 7.5 | 7 | 8.1 | 8.6 | 8.3 |
| MCV | 63 | 68 | 69 | 70 | 73 | 74 | 73 |
| Platelet count | 180 | 221 | 408 | 562 | 413 | 385 | 385 |
| WBC count | 10.7 | 26.8 | 15.1 | 37.7 | 17.4 | 12.8 | 10.4 |
| Neutrophil | 82 | 90 | 93 | 93 | 89 | 73 | 68 |
| Lymphocyte | 14 | 6 | 4 | 3 | 8 | 22 | 25 |
| D1 | D3 | D7 | D10 | D15 | D20 | D21 | |
| Blood urea nitrogen (bun) | 9 | 13 | 8 | 10 | |||
| Urea | 19.3 | 27.8 | 17.1 | 21.4 | |||
| Creatinine | 0.62 | 0.55 | 0.49 | 0.48 | |||
| Sodium | 138 | 139 | 137 | 138 | 138 | 137 | 138 |
| Potassium | 3.7 | 2.9 | 2.8 | 3.2 | 4 | 4.2 | 3.8 |
| Chloride | 98 | 102 | 99 | 101 | 107 | 102 | 103 |
| Calcium total | 7.4 | 7.6 | 7 | 8.1 | |||
| D1 | D3 | D7 | D10 | ||||
| Bilirubin direct | 0.5 | 0.3 | 0.2 | 0.3 | |||
| Bilirubin indirect | 0.5 | 0.5 | 0.3 | 0.3 | |||
| Albumin | 2.9 | 3 | 2.4 | 2.9 | |||
| Globulin | 3.1 | 2.6 | 3.1 | 2.7 | |||
| AST | 18 | 54 | 18 | 18 | |||
| ALT | 17 | 32 | 22 | 15 | |||
| Alkaline phosphatase | 53 | 84 | 98 | 80 | |||
| INR | 1.48 | 1.44 | 1.24 | ||||
| SARS-CoV-2 (COVID-19) Real Time PCR | Negative | ||||||
| Viral markers | Negative | ||||||
| ABG | D1 | D3 | D7 | D14 | D18 | D20 | |
| pH | 7.44 | 7.46 | 7.52 | 7.49 | 7.47 | 7.44 | |
| pCO2 | 32 | 33 | 35 | 38 | 39 | 42 | |
| pO2 | 116 | 162 | 162 | 153 | 131 | 110 | |
| Lactate | 1.5 | 3 | 1.9 | 2.4 | 1.4 | 2.2 | |
| HCO3 | 21.7 | 23.5 | 28.6 | 29 | 28.4 | 28.5 | |
| Pleural fluid examination | |||||||
| Biochemical analysis | |||||||
| Glucose | 119 | ||||||
| Protein | 3.6 | ||||||
| Cytology | |||||||
| TCC | 1024 cells /cumm | ||||||
| DLC | Mononuclear - 30%, Polymorphs - 70% | ||||||
| RBC | 12000 cells /cumm | ||||||
| Culture/sensitivity | NO GROWTH | ||||||
| ADA | 24.6 | ||||||
| TB PCR | Negative | ||||||
| Lactate dehydrogenase (serum) | 388 | ||||||
| Lactate dehydrogenase (pleural fluid) | 758 | ||||||
| D10 | |||||||
| D-dimer | 5 | ||||||
| D14 | |||||||
| C reactive protein | 139.05 | ||||||
| Bal examination | |||||||
| Culture/sensitivity | No growth | ||||||
| Fungal culture/sensitivity | Candida albicans - Sensitive to Fluconazole, Ketoconazole, Voriconazole, Cotrimazole | ||||||
| Cytology | Smears show endobronchial cells, metaplastic cells, squamous cells, macrophages, neutrophils, lymphocytes, RBCs, no malignant cells | ||||||
Pyrethroid poisoning primarily affects the nervous system by acting on voltage-sensitive sodium channels, delaying their closure and causing prolonged depolarisation. This mechanism is the basis of the toxic effects seen in the excitable cells of the nervous and muscular systems. In this case, the respiratory symptoms, including breathlessness and chest pain, along with bilateral pleural effusion, point to an acute lung injury likely caused by a hypersensitivity reaction in the lung tissue. These findings are consistent with prior studies showing that pyrethroids, particularly Type II compounds like prallethrin, can lead to respiratory symptoms, hypersensitivity reactions, and neurological effects [1,7].
The clinical management of this case involved a combination of supportive care, symptomatic treatment, and specific interventions to address the respiratory complications. The patient required non-invasive ventilation and pigtail catheter insertion to manage pleural effusion, which significantly contributed to her respiratory distress [5]. Pleural drainage was a key intervention, as it relieved the pressure on the lungs, allowing for improved respiratory function. The pigtail catheter offers reliable treatment of effusions and is a safe and less invasive alternative to tube thoracostomy [8]. This highlights the importance of early and aggressive management of respiratory complications in pyrethroid poisoning.
Symptomatic treatment in this case included broad-spectrum antibiotics, antifungals based on culture results, and corticosteroids, although the latter remains controversial in pyrethroid poisoning cases [4]. The decision not to use corticosteroids early in the treatment was based on existing literature that offers mixed evidence regarding their efficacy in treating pyrethroid-induced lung injury. Nevertheless, the patient showed clinical improvement, reinforcing the effectiveness of supportive measures without the need for high-dose steroids.
Bronchoscopy and Bronchoalveolar Lavage (BAL) played important diagnostic roles, revealing excessive secretions and a secondary fungal infection (Candida albicans), which may have compounded the patient’s respiratory issues. The use of intravenous atropine to control excessive secretions [6], a common complication in severe pyrethroid poisoning along with regular nebulization and chest physiotherapy to maintain airway patency. Atropine can be used independently for anti-salivation effects, Intravenous (IV) atropine indications include patients with hypersalivation and bronchial secretions [9].
This case emphasizes the importance of thorough exposure history in identifying the cause of poisoning, especially in environments where pyrethroid-containing products are readily available. The non-specific nature of the clinical presentation, combined with the rarity of pyrethroid poisoning in humans, can lead to diagnostic challenges, particularly in differentiating it from more common toxicological and infectious conditions. In the absence of a specific antidote for prallethrin poisoning, timely symptomatic management remains the cornerstone of treatment.
Conclusion
This case report highlights a rare instance of prallethrin poisoning, emphasizing the need for swift recognition, comprehensive supportive care, and thorough monitoring in manag- ing pyrethroid toxicity. The patient’s recovery underscores the importance of a multidisciplinary ICU approach, including BiPAP support for respiratory distress, pigtail insertion for pleural effusion, and atropine administration to control excessive secretions.
Prallethrin, commonly found in household insecticides like All Out, can cause diverse symptoms, complicating diagnosis. The patient’s respiratory distress and pleural effusion were initially challenging to differentiate from other conditions like infections. A thorough diagnostic process, including vital sign assessment, imaging, and pleural fluid analysis, was crucial in confirming pyrethroid toxicity.
The tailored treatment plan, combining respiratory support, drainage, atropine, antibiotics, antifungals, and nebulization, played a key role in the patient’s recovery. This case underscores the importance of early recognition, thorough exposure history, and personalized care in managing pyrethroid poisoning effectively.
Declarations
Funding: No funding was received.
Conflict of interest: The authors declare no conflict of interest.
References
- Bradberry SM, Cage SA, Proudfoot AT, Vale JA. Poisoning due to pyrethroids. Toxicol Rev. 2005; 24: 93-106.
- Ramchandra AM, Victor PJ. Pyrethroid Poisoning. Indian J Crit Care Med. 2019: 23.
- Glickman AH, Casida JE. Species and structural variations affecting pyrethroid neurotoxicity. Neurobehavioral Toxicology and Teratology. 1982, 4:793-799.
- Chandra Alka, Dixit Madhu B, Banavaliker Jayant N. Prallethrin poisoning: A diagnostic dilemma. Journal of Anaesthesiology Clinical Pharmacology. 2013; 29: 121-122.
- Soderlund DM. Molecular mechanisms of pyrethroid insecticide neurotoxicity: recent advances. Arch Toxicol. 2011; 165-181.
- Ray DE, Forshaw PJ. Pyrethroid insecticides: poisoning syndromes, synergies, and therapy. J Toxicol Clin Toxicol. 2000; 95-101.
- Dorman DC, Beasley VR. Neurotoxicology of pyrethrin and the pyrethroid insecticides. Vet Hum Toxicol. 1991; 33: 238-243.
- Mehta AA, Gupta AS, Mohamed AKS. The Pigtail Catheter for Pleural Drainage: A Less Invasive Alternative to Tube Thoracostomy. Journal of Current Surgery. 2016; 4: 52-6.
- McLendon K, Preuss CV. Atropine. In. StatPearls [Internet (ed): Treasure Island (FL): StatPearls Publishing. 2024; 2024: 19.