
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Diaphragmatic strictures secondary to chronic NSAID use
Ankit Agarwal; Chhagan Lal Birda; Ashish Agarwal*
Department of Gastroenterology, All India Institute of Medical Sciences, Jodhpur, India.
*Corresponding Author : Ashish Agarwal
Associate Professor, Department of Gastroenterology,
All India Institute of Medical Sciences, Jodhpur, India.
Email: drashu123@gmail.com
Received : Jan 24, 2025
Accepted : Feb 19, 2025
Published : Feb 26, 2025
Archived : www.jcimcr.org
Copyright : © Agarwal A (2025).
Citation: Agarwal A, Birda CL, Agarwal A. Diaphragmatic strictures secondary to chronic NSAID use. J Clin Images Med Case Rep. 2025; 6(2): 3485.
Description
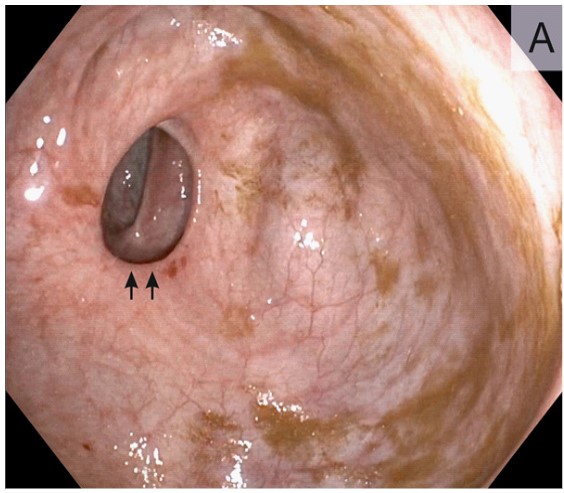
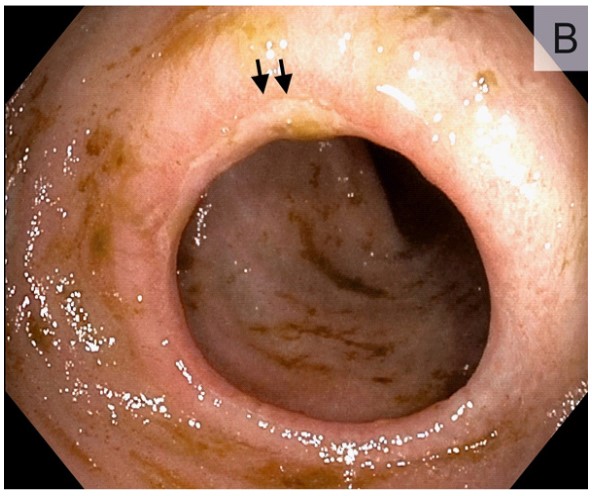
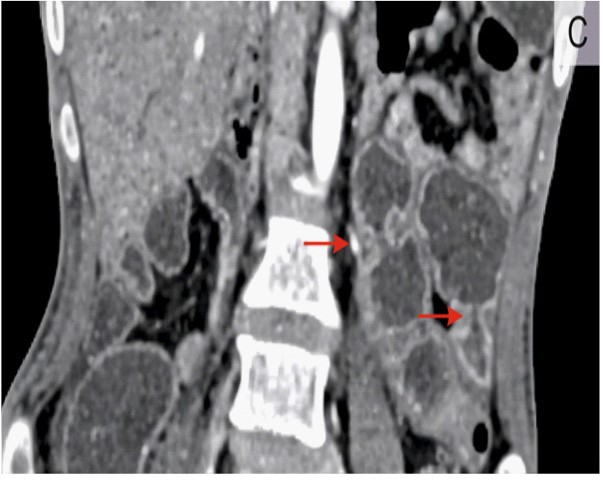
A 27-year-old male presented to the gastroenterology clinic with a 3-year history of abdominal pain and easy fatigability. On physical examination, there were bilateral large and small joint deformities. Medication history was notable for daily ingestion of over-the-counter tablet diclofenac (100 mg) twice daily for more than 15 years for joint pain. Laboratory testing revealed anemia (hemoglobin 8.7 g/dl, [reference 11-15 g/dl]) and hypoalbuminemia (3.1 g/dl, [reference 3.5-5.0 g/dl]). Upper gastrointestinal endoscopy was normal. Colonoscopy showed presence of diaphragm-like strictures in the ascending colon (Figure 1) and terminal ileum (Figure 2). Computed tomography (CT) of the abdomen showed multifocal short-segment strictures in jejunum and ileum (Figure 3, Arrow). Colonic biopsies were unremarkable. A diagnosis of NSAID enteropathy secondary to RF-negative polyarticular juvenile idiopathic arthritis was made. NSAID enteropathy is an entity that occurs due to long term ingestion of NSAIDs [1]. Diagnosis requires the exclusion of other causes of stricture formation, particularly Crohn’s disease [2]. Management includes discontinuation of NSAID’s [3]. Patient was started on steroids and iron supplementation in consultation with rheumatology team. After 6 weeks anemia improved and steroids were tapered and switched to steroid sparing agents.
Declarations
Contributors: CLB, AA treated the patient. AA drafted the manuscript. AA provided critical revision of the report. All authors reviewed and approved the final version.
Competing interests: We declare no competing interests.
References
- Shin SJ, Noh CK, Lim SG, Lee KM, Lee KJ. Non-steroidal anti- inflammatory drug-induced enteropathy. Intest Res. 2017; 15: 446–55.
- Lim YJ, Yang CH. Non-steroidal anti-inflammatory drug-induced enteropathy. Clin Endosc. 2012; 45: 138–44.
- Lim YJ, Chun HJ. Recent Advances in NSAIDs-Induced Enteropathy Therapeutics: New Options, New Challenges. Gastroenterol Res Pract. 2013; 2013: 1–7.