
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 6
Exploring choroidal tuberculoma: Insights from a case series
Sonal Paliwal1*; Shubra Thakkar2; Sonu Shukla3
1Vitreo Retina Consultant, Sewa Sadan Eye Hospital, India.
2DNB Resident, Sewa Sadan Eye Hospital, India.
3Optometrist, Sewa Sadan Eye Hospital, India.
*Corresponding Author : Sonal Paliwal
Vitreo Retina Consultant, Sewa Sadan Eye Hospital,
Bhopal, India.
Tel: 9866711809
Email: sonal22paliwal@gmail.com
Received : Jan 24, 2025
Accepted : Feb 19, 2025
Published : Feb 26, 2025
Archived : www.jcimcr.org
Copyright : © Paliwal S (2025).
Abstract
Background: Management of intraocular tuberculosis is a challenge due to its varied manifestations, lack of uniform diagnostic criteria and treatment protocols. Here in we present 4 cases of Tubercular granuloma successfully treated with anti – tubercular drugs along with systemic steroids.
Purpose: To report a series of 4 cases of tubercular choroidal granuloma along with its clinical spectrum, management, and prognosis.
Method: Retrospective data of four patients diagnosed with tubercular choroidal granuloma on the basis of clinical presentation, highly positive tuberculin skin test, positive IGRA test (Interferon-Gamma Release Assays) and a positive response to anti-tubercular drugs along with systemic steroids was analysed.
Results: Amongst all 4 patients presenting with a yellowish mass lesion one patient was already a diagnosed case of Tuberculosis and was on anti-tubercular drugs. All four patients responded completely to anti-tubercular drugs along with systemic steroids with improvement in visual acuity and decrease in the size of lesion.
Conclusion: Intraocular tuberculosis can manifest as choroidal granulomas. Oral anti-tubercular drugs along with systemic steroids helps to improve vision and prevent relapse in these cases.
Keywords: Ocular tuberculosis; Choroidal granuloma; Anti-tubercular drugs; Steroids.
Citation: Paliwal S, Thakkar S, Shukla S. Exploring choroidal tuberculoma: Insights from a case series. J Clin Images Med Case Rep. 2025; 6(2): 3486.
Introduction
Ocular Tuberculosis (TB) is one of the common (0.4-9.8%) extrapulmonary manifestation of Mycobacterium tuberculosis infection, which can affect various structures of the eye [1]. Intraocular tuberculosis is a great mimicker of various uveitis entities. Amongst the various ocular structures, most common clinical presentation includes posterior uveitis followed by anterior uveitis, panuveitis and intermediate uveitis. Among these manifestations, choroidal granulomas represent a unique clinical entity characterized by localized inflammation in the choroid.
The diagnosis of Tubercular choroidal granuloma involves a combination of clinical suspicion, imaging modalities such as Optical Coherence Tomography (OCT) and Fundus Fluorescein Angiography (FFA), and confirmatory investigations like Polymerase Chain Reaction (PCR), Interferon-Gamma Release Assays (IGRA), chest X ray, computerized tomography or biopsy in selected cases. The management typically requires a combination of Anti-Tubercular Therapy (ATT) and adjunctive corticosteroids, tailored to the severity and extent of ocular involvement. However, the heterogeneous presentations of choroidal granulomas demand an individualized approach to diagnosis and treatment.
The absence of clinical manifestation of pulmonary TB does not exclude the possibility of ocular TB, due to the fact that around 60% of patient with extrapulmonary TB have no signs of pulmonary TB [2].
In this case series, we report four cases of ocular TB presenting with choroidal granulomas. These cases highlight the varied presentations of this condition, emphasizing the importance of a high index of suspicion and a thorough workup to ensure timely and accurate diagnosis. By documenting the clinical features, diagnostic pathways, and therapeutic outcomes of these cases, we aim to contribute to the growing body of literature on ocular TB and enhance awareness among clinicians regarding this enigmatic disease entity.
Materials and methods
This is a retrospective observational case series from a tertiary referral eye institute in central India. We evaluated data of 4 patients who were diagnosed and treated as Tubercular choroidal granuloma.
Complete ophthalmological evaluation including Best Corrected Visual Acuity (BCVA), Intraocular Pressure (IOP), anterior and posterior segment evaluation, optical coherence tomography was done. If possible, fundus fluorescence angiography was also done.
Investigations included a CBC (complete blood count), ESR (erythrocyte sedimentation rate), Human Immunodeficiency Virus (HIV), Hepatitis B Surface Antigen (HBsAg), Venereal Disease Research Laboratory test (VDRL), Mantoux test and TB Gold test (Interferon-gamma release assay or IGRA). Radiological investigations included chest x ray and HRCT-Chest if feasible.
The research adhered to the tenets of the Declaration of Helsinki and informed consent from patients was taken.
Case 1
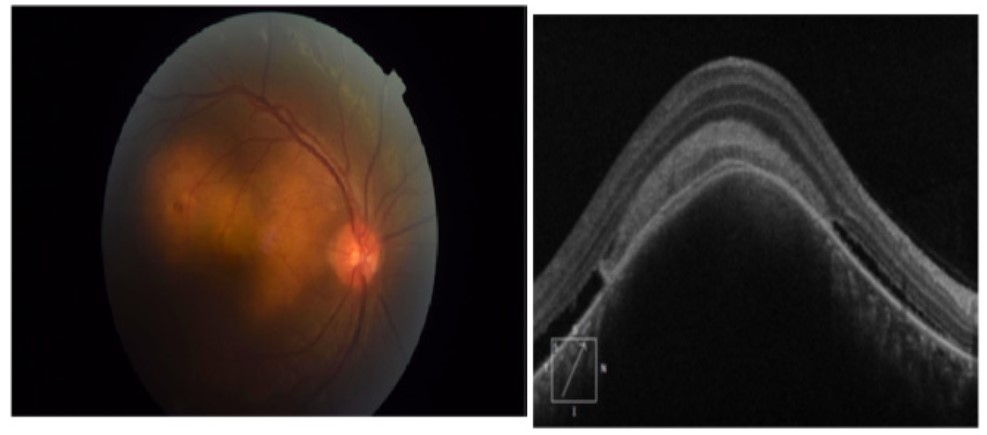
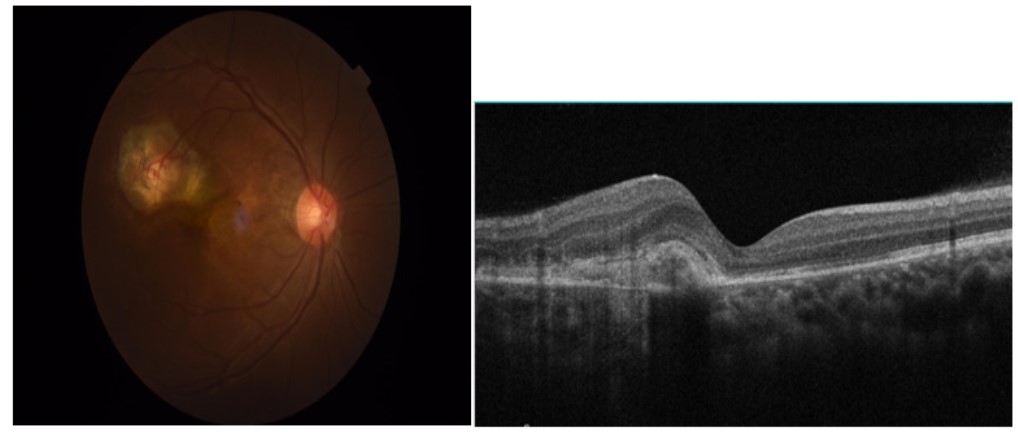
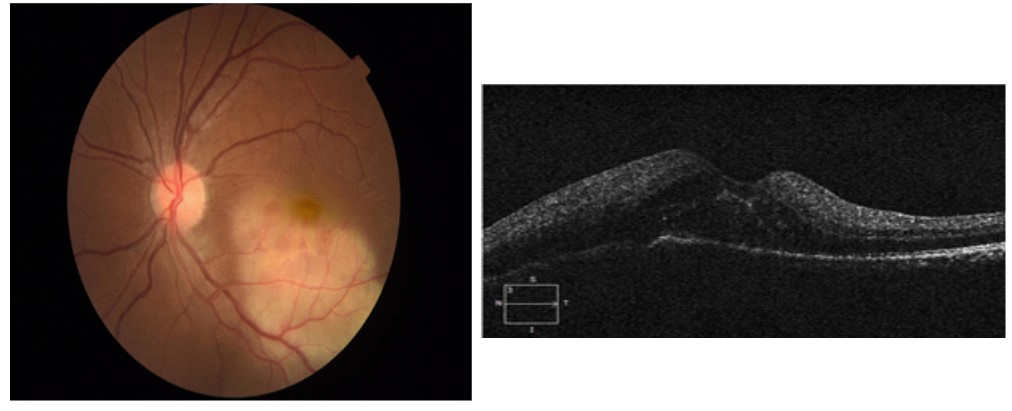
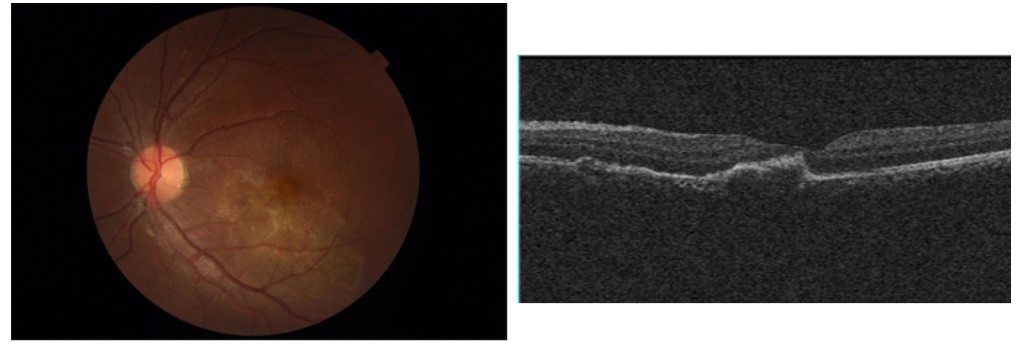
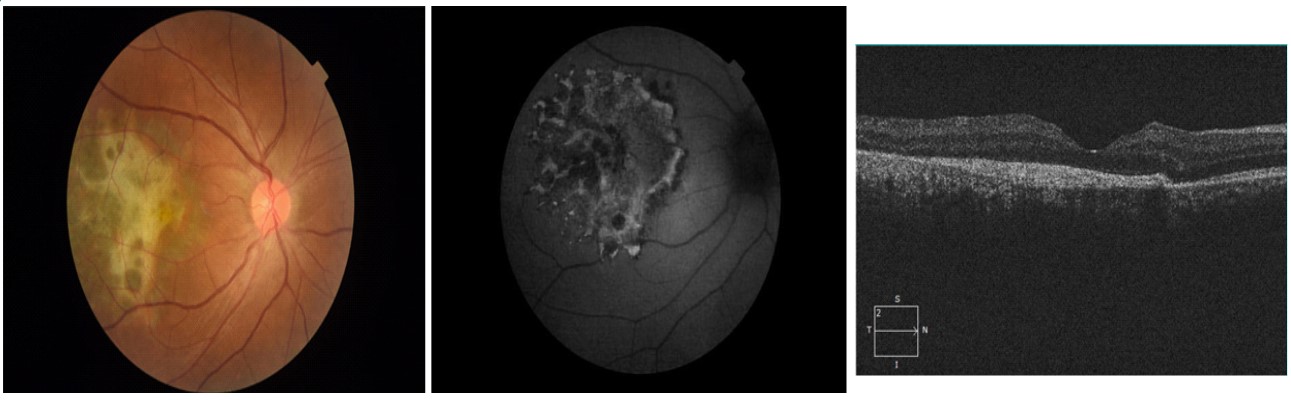
27-year-old female, known case of pulmonary TB since 3 months, was on ATT, compliant with treatment came with the complains of painless, gradual diminution of vision in right eye since 1 month. She had no complains in the left eye. On examination, her visual acuity was CF in right eye and 6/6 in left eye. Her IOP was 14 mmHg and 15 mmHg in right and left eye respectively. On clinical examination of the right eye, her anterior segment was quiet, fundus showed a yellowish elevated mass lesion at the macula. On SD-OCT, a large choroidal granuloma with subretinal fluid was seen (Figure 1). Left eye examination was found to be within normal limits. She was started on oral prednisolone at 1 mg/kg body weight in tapering doses for 2 months. She was reviewed by her chest physician to rule out MDR-TB. However, MDR-TB was ruled out and her course of ATT was extended to 9 months in view of extrapulmonary manifestations. At the end of 2 months, her visual acuity has improved to 6/60 along with resolution of granuloma. An oral dose of prednisolone 5 mg is continued for another 2 months. Her vision is maintained at 6/36 with scarring at macula after 5 months of completing AKT (Figure 2).
Case 2
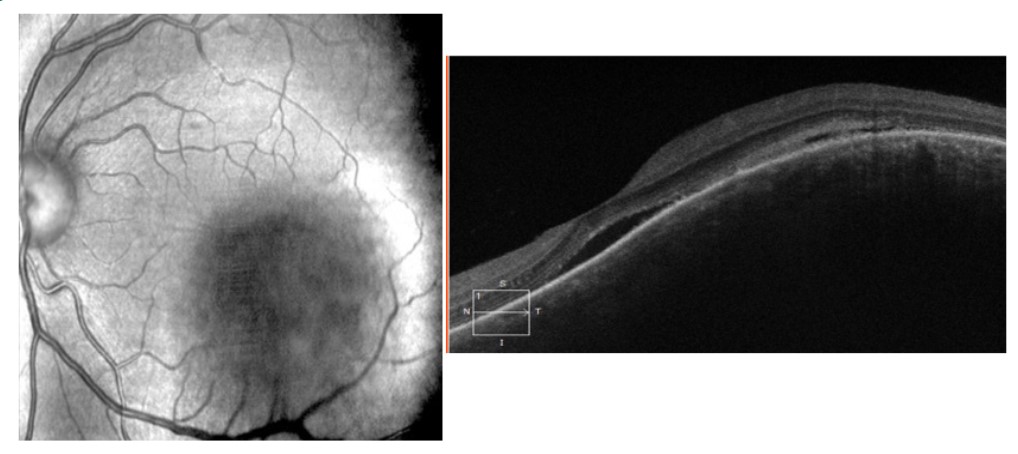
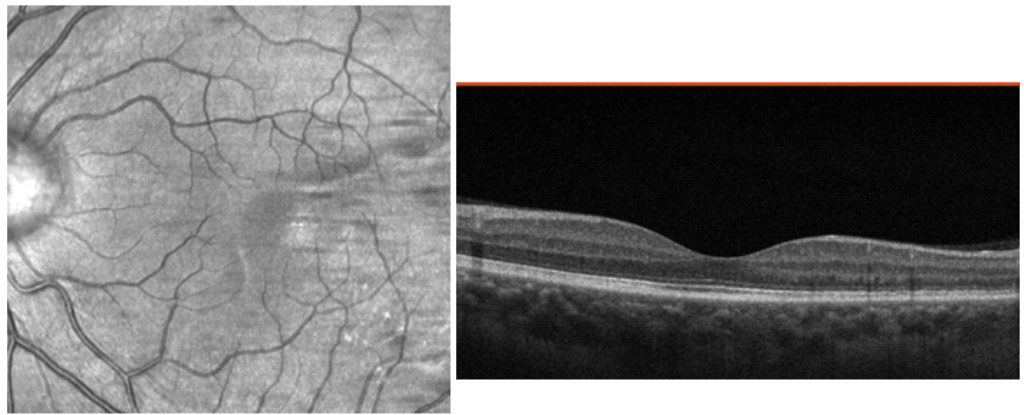
34-year-old female presented to the outpatient department with complains of mild redness, pain and decreased vision in her left eye which she observed in the past 1 week. Her visual acuity was 6/6 in the right eye and 6/36 in the left eye, IOP was 15 and 21 mmHg in the right and left eye respectively. On examination, of her left eye she had conjunctival congestion with few cells in anterior chamber. On fundus examination, there was a yellowish lesion of approximately 4x4 mm in the inferotemporal quadrant involving macula. The disc and periphery were within normal limits. On OCT, a choroidal granuloma with subretinal fluid was seen (Figure 3). Her right eye was quiet externally and the fundus examination was within normal limits. She was started on topical prednisolone acetate four times a day, tapered weekly. She was also advised a uveitis profile. Her investigations turned out positive for QuantiFERON TB gold and Tuberculin skin testing. Other investigations were negative. She was reviewed with a chest physician suspecting a case of TB granuloma and ATT was started. She was also started on oral prednisolone 1 mg/kg body weight tapered over 2 months. Her vision returned to 6/6 with the subsidence of granuloma and sub retinal fluid after 4 months of treatment (Figure 4). She is continued on AKT for 9 months. Patient remained stable at one year follow up after starting AKT.
Case 3
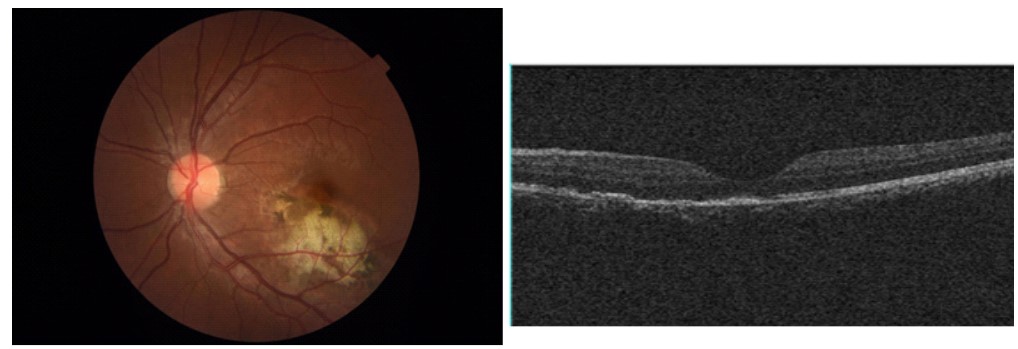
24-year-old male, presented to the OPD with diminution of vision in the left eye for 15 days. No such complaints were noted in the right eye. His visual acuity in right eye was 6/6 and in left eye was 5/60. IOP was 20 mmhg in both eyes. Right eye examination was completely within normal limit. On examination of the left eye, anterior segment was quiet. Fundus examination showed a yellowish elevated lesion beneath the macula with subretinal hemorrhage (Figure 5). Serological profile was advised and Mantoux test, QuantiFERON TB Gold were found to be positive. The patient was referred to pulmonologist for initiating Anti Tubercular Therapy. Oral prednisolone 1 mg/ kg was started and then tapered weekly. He was monitored close- ly. The granuloma started resolving with improvement in vision. At 2 weeks of treatment, his vision in left eye improved to 6/18 (Figure 6). At 4th week of treatment, the granuloma resolved completely with punched out scarring at the macula. His vision returned to 6/6. At the end of 9 months after completion of course of ATT, his vision is maintained at 6/6 (Figure 7). The patient remained stable with no recurrences in subsequent follow ups up to one year of treatment.
Case 4
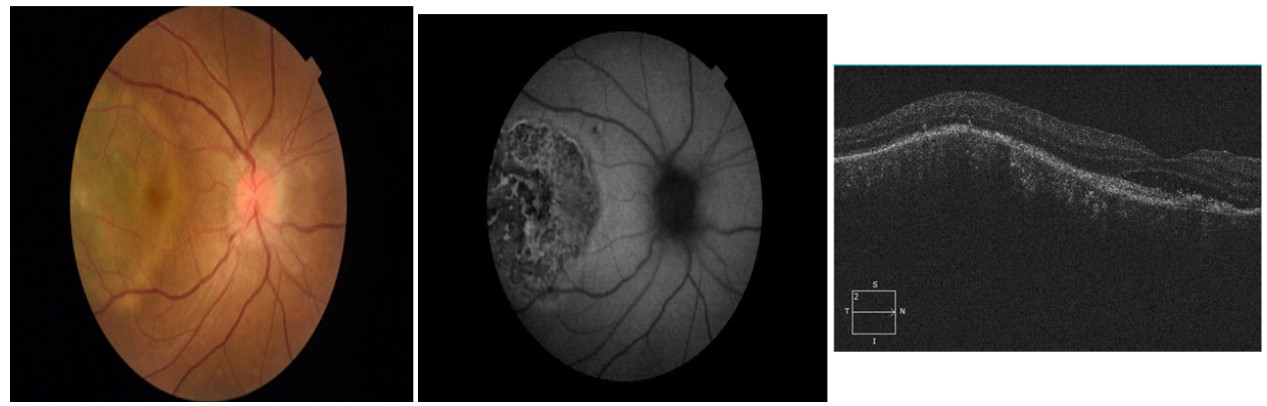
44-year-old female, presented with diminution of vision in right eye noticed in the past 8 days. Her visual acuity in the right eye was finger counting and in left eye was 6/6. Her IOP was 10 mmHg and 12 mmHg in right and left eye respectively. On examination, anterior segment in right eye was quiet. Fundus examination showed disc edema and yellowish mass like lesion in the temporal quadrant involving macula. OCT showed presence of choroidal granuloma (Figure 8). The examination of her left eye revealed no abnormalities. Amongst all investigations advised Mantoux and QuantiFERON TB gold turned out to be positive. The patient was started on oral prednisolone acetate 1 mg/kg body weight tapered weekly, along with Anti Tubercular Therapy after consulting chest physician. She took complete course of ATT for 9 months. The disc edema subsided gradually after initiating therapy. At 1 year follow up, granuloma healed along with scarring at the macula with vision being maintained at 1/60 (Figure 9).
Results
Diagnosis of TB granuloma was made on the basis of compatible clinical picture along with highly positive TST (>15 MM) and positive IGRA test. All patients were treated with a course of Anti-tubercular drugs along with oral steroids in tapering doses. Patients were followed up for at least one year and a complete ocular evaluation was done at every visit. All patients showed a complete resolution of granuloma with improvement in visual acuity. All of our patients remained stable with no recurrences in subsequent follow ups.
Discussion
Choroidal granuloma is a rare but sight threatening presentation of tuberculosis. This case series highlights the diverse presentations and management of granulomas. Our patients range from 24 to 67 years demonstrating that this condition can manifest across a wide age spectrum.
The first case is particularly significant due to its unique aspect, as the patient developed a granuloma despite being on Antitubercular Therapy. It underscores the importance of incorporating steroids in the management of granulomas, even though some reports suggest that ATT monotherapy may be sufficient for their treatment [3]. The second case is distinctive because of the rare primary presentation of tuberculosis as a choroidal granuloma in a young female. Its resolution and complete visual recovery with combined steroids and ATT provide an encouraging outcome. The last two cases reinforce the value of early presentation, prompt medical attention and adherence to treatment.
Intraocular Tuberculosis is a type of extrapulmonary TB seen in an TB endemic country like India. It has been reported that in 6.8% of the patients with pulmonary TB ocular involvement is seen [4]. Diagnosis and management of TB Uveitis still remains controversial due to scarcity of clinical trials.
Recently Collaborative ocular tuberculosis study consensus guidelines on management of tubercular uveitis have provided with evidence and experienced based recommendations on management of tubercular uveitis [5]. According to the guidelines, AKT Can be started in TB granuloma if the clinical features are suggestive of TB aetiology and one of the immunological tests is positive. In all of our cases, clinical features were suggestive of choroidal tuberculoma which are typically larger solitary yellowish lesion (up to 7 mm in diameter) with well-defined margins [6]. In all the cases Mantoux test was highly positive along with TB-gold positive. All the patients were treated with AKT along with oral steroids. Good resolution of granuloma with recovery of vision was noted which was maintained after one year of initiating therapy with no recurrences seen.
Use of steroids in treating TB Uveitis is a controversial topic. A metanalysis reported no significant difference in treatment outcomes with or without systemic corticosteroids use in patients treated with ATT [7]. However, it is the timing of starting steroids which is important. According to a cohort study, physician should delay prescribing systemic corticosteroids until after initiating of ATT in patients with high clinical suspicion of TB Uveitis unless there is a high risk of complication secondary to intense inflammatory reaction [8]. The presentation of choroidal tuberculoma even on being AKT for 3 months in the first case and the larger size of the lesions in all the cases prompted us to start steroids along with AKT. In all our patient’s steroids were started after initiating of AKT.
The presence of choroidal involvement and vitreous haze was associated with a higher risk of recurrence [8]. Manifestation hypothesized to be an autoimmune reaction as opposed to direct infection by TB bacilli. This difference between an auto-immune and infectious causes of various TB Phenotypes in eye will help us understand the role of ATT and corticosteroids in the treatment of patients with TB uveitis.
Unusual case of TB Choroiditis well treated with AKT and oral steroids have been reported in literature before [9,10].
Conclusion
Ocular tuberculosis can present with varied manifestation involving anterior and posterior segment. A high index of suspicion should be kept in mind while dealing with any type of ocular inflammation specially in a endemic country like India. We recommend to start with Anti-TB medication in cases with highly positive TST or a positive IGRA test along with a compatible clinical picture. Oral steroids should be started after starting AKT to avoid confusion in clinical course of the disease. AKT should be continued at least till 6 months or more according to the severity of clinical presentation. Although controlled clinical trials supporting the exact pathogenesis and management of tubercular uveitis are needed our case series may add to the scarce literature leading to early diagnosis with better outcomes.
References
- Gupta V, Gupta A, Rao NA. Intraocular tuberculosis--an update. Surv Ophthalmol. 2007; 52: 561-87.
- Alvarez S, McCabe WR. Extra pulmonary tuberculosis revisited: A review of experience at Boston City and other hospitals. Medicine (Baltimore) 1984; 63: 25–55.
- Khalsa A, Kelgaonkar A, Basu S. Anti-TB monotherapy for choroidal tuberculoma: an observational study. Eye (Lond). 2022; 36: 612-618.
- Lara LP, Ocampo V, Jr Prevalence of presumed ocular tuberculosis among pulmonary tuberculosis patients in a tertiary hospital in the Philippines. J Ophthalmic Inflamm Infect. 2013; 3: 1.
- Agrawal R, Testi I, Mahajan S, Yuen YS, Agarwal A, Kon OM, et al. Collaborative Ocular Tuberculosis Study Consensus Group. Collaborative Ocular Tuberculosis Study Consensus Guidelines on the Management of Tubercular Uveitis-Report 1: Guidelines for Initiating Antitubercular Therapy in Tubercular Choroiditis. Ophthalmology. 2021; 128: 266-276.
- Albert DM, Raven ML. Ocular Tuberculosis. Microbiol Spectr. 2016; 4.
- Kee AR, Gonzalez-Lopez JJ, Al-Hity A, Gupta B, Lee CS, Gunasekeran DV, et al. Anti-tubercular therapy for intraocular tuberculosis: A systematic review and meta-analysis. Surv Ophthalmol. 2016; 61: 628-53.
- Agrawal R, Gunasekeran DV, Grant R, et al. Clinical Features and Outcomes of Patients with Tubercular Uveitis Treated with Antitubercular Therapy in the Collaborative Ocular Tuberculosis Study (COTS)–1. JAMA Ophthalmol. 2017; 135: 1318–1327.
- Aggarwal K, Agarwal A, Sehgal S, et al. An unusual presentation of intraocular tuberculosis in a monocular patient: clinicopathological correlation. J Ophthal Inflamm Infect. 2016; 6: 46.
- Singh A, Singh BK, Singh VK, Nagarajan S. Presumptive ocular tuberculosis: A case series of rare cases. Oman J Ophthalmol. 2023; 16: 529-532.