
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Radiological presentation of large arachnoid cyst: Clinical image
Swati Vijapurkar1; Monica Khetarpal2; Jitendra V Kalbande3; Gade Sandeep1; Jakkireddy Sravani1*
1Senior Resident, Department of Anaesthesia, All India Institute of Medical Sciences, India.
2Professor, Department of Anaesthesia, All India Institute of Medical Sciences, India.
3Associate Professor, Department of Anaesthesia, All India Institute of Medical Sciences, India
*Corresponding Author : Jakkireddy Sravani
Senior Resident, Department of Anaesthesia, All
India Institute of Medical Sciences, Raipur, India
Email: sravanijakkireddy115@gmail.com
Received : Jan 22, 2025
Accepted : Feb 20, 2025
Published : Feb 27, 2025
Archived : www.jcimcr.org
Copyright : © Sravani J (2025).
Citation: Vijapurkar S, Khetarpal M, Kalbande JV, Sandeep G, Sravani J. Radiological presentation of large arachnoid cyst: Clinical image. J Clin Images Med Case Rep. 2025; 6(2): 3487.
Description
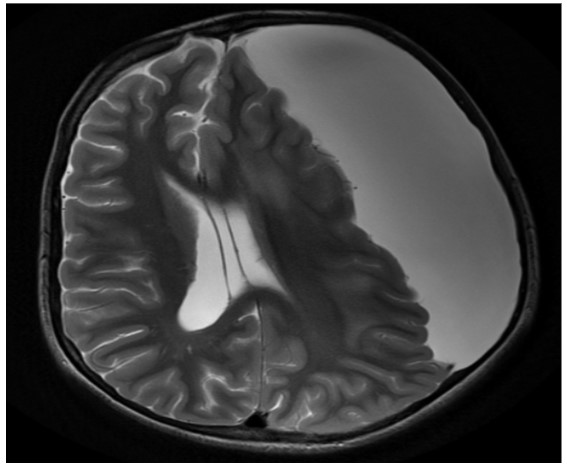
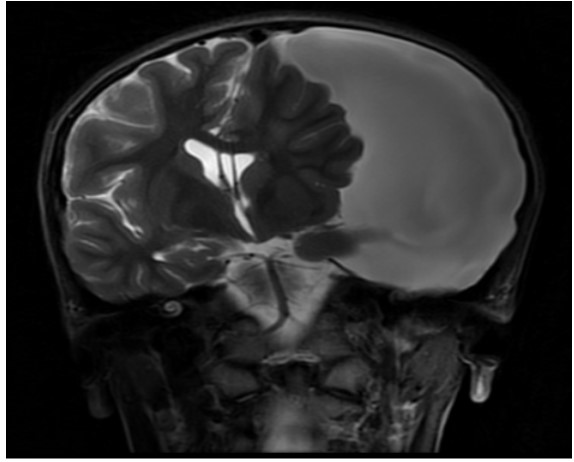
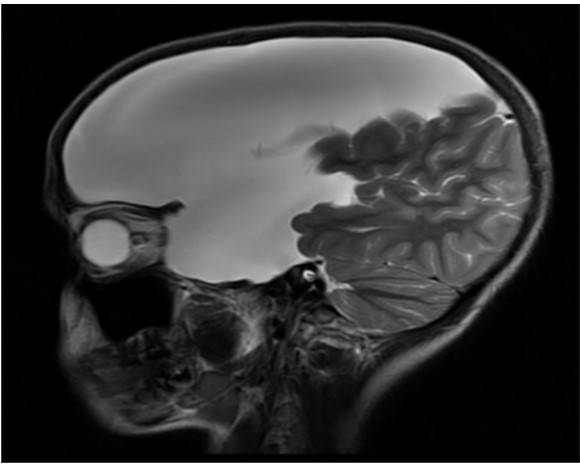
A 13-year-old male child weighing 36 kg presented with complaints of abnormal jerky movements of upper limbs and lower limbs, two episodes in the last month. It was associated with uprolling of eyes and incontinence of urine. After clinical evaluation, the patient was started on Inj Levitriacetam 250 mg and baseline investigations were ordered. The blood investigations were within normal limits. On Magnetic Resonance Imaging (MRI), a large extra-axial thin-walled cystic lesion, measuring 15×5.2×11.6 cm (APxTRxCC) was noted in left supratentorial compartment along the left frontal, temporal and parietal convexity, extending inferiorly to the middle cranial fossa. The lesion is homogeneously hyper-intense on T2 (Figures 1-3) and shows complete suppression on FLAIR. The lesion resulted in significant mass effect on the left cerebral parenchyma with contralateral displacement of left frontal, temporal and parietal lobes, and midline shift to the right by ~10 mm and scalloping of the overlying calvarium. A diagnosis of a large arachnoid cyst with significant mass effects was made and the patient was planned for craniotomy and decompression of the cyst. General anaesthesia with endotracheal intubation was administered and the surgery was uneventful. The patient was extubated in the Operation Room (OR).
An arachnoid cyst is a fluid-filled sac that develops between the brain or spinal cord and the arachnoid mater. These cysts are usually filled with Cerebrospinal Fluid (CSF) and are often congenital. However, they can also be acquired due to trauma, infection, or surgery. They are benign and mostly located near the temporal lobe or cerebellum. Many arachnoid cysts are asymptomatic and discovered incidentally. However, if the cyst grows or exerts pressure on surrounding structures, symptoms may occur. Neurological symptoms like headache, seizures, dizziness, or vision problems; motor symptoms like weakness, or balancing issues. Other symptoms like nausea, vomiting, or developmental delays may be seen in children. Small, asymptomatic cysts may require regular monitoring with imaging. For symptomatic or growing cysts, procedures like fenestration, shunting, or minimally invasive techniques such as endoscopic procedures may be performed to manage the cyst.
References
- Pradilla G, Jallo G. Arachnoid cysts: case series and review of the literature. Neurosurg Focus. 2007; 22: E7.
- Bang JS, Oh CW, Kim MS, et al. Two Cases of Intraventricular Arachnoid Cysts: Case Report. Journal of Korean Neurosurgical Society. 2025; 30: 928-933.