
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Extracorporeal support and hemoadsorption with Cytosorb in hemophagocytic lymphohistiocytosis syndrome secondary to HIV
Paola Borbolla-Flores1; Juan Pablo Gómez-Villarreal1; Ricardo Garza-Treviño1; Rolando Claure-Del Granado2; Lilia M Rizo-Topete1*
1Department of Internal Medicine and Nephrology, UDEM-Christus Muguerza High Specialty Hospital, Mexico.
2Division of Nephrology, School of Medicine, IIBISMED, Hospital Obrero No. 2 - CNS, Major University of San Simón, Bolivia.
*Corresponding Author : Lilia María Rizo-Topete
Department of Internal Medicine and Nephrology,
Universidad de Monterrey, Hospital Christus
Muguerza Alta Especialidad, Hidalgo 2525,
Monterrey, Nuevo León, 64000, México.
Tel: +52-818-399-3400;
Email: lilia.rizo@udem.edu
Received : Jan 27, 2025
Accepted : Feb 21, 2025
Published : Feb 28, 2025
Archived : www.jcimcr.org
Copyright : © Rizo-Topete LM (2025).
Abstract
Introduction: Hemophagocytic Lymphohistiocytosis (HLH) is an aggressive and life-threatening syndrome of excessive immune activation. It can be secondary to multiple etiologies and lead to multi-organ failure. The kidneys are one of the main organs affected, causing Acute Kidney Injury (AKI). Typically, patients who present with multi-organ failure are critically ill and require care in the Intensive Care Unit (ICU). The primary treatment provided by nephrology is extracorporeal support. Hemoadsorption can reduce inflammatory cytokines and serve as a bridge to treatment for the underlying etiology causing HLH.
Objectives: To evaluate the improvement in multiple laboratory parameters in patients with multi-organ failure secondary to HLH treated with hemoadsorption.
Methodology: We present a clinical case of a young patient who developed HLH secondary to a recently diagnosed HIV infection. The patient presented with Multi-Organ Dysfunction Syndrome (MODS), including Acute Kidney Injury (AKI). Extracorporeal support with Continuous Renal Replacement Therapy (CRRT) and hemoadsorption with CytoSorb was applied successfully for three sessions. After therapy discontinuation, the patient’s clinical condition deteriorated, ultimately leading to death.
Results: Hemoadsorption effectively reduced elevated total bilirubin (due to liver failure), albumin, and creatinine levels, achieving a more physiological state as a bridge for the treatment of the underlying etiology, HIV, and superinfections.
Keywords: AKI; Hemoadsorption; CytoSorb; HIV; HLH.
Citation: Borbolla-Flores P, Gomez-Villarreal JP, Garza-Trevino R, Granado RCD, Rizo-Topete LM. Extracorporeal support and hemoadsorption with Cytosorb in hemophagocytic lymphohistiocytosis syndrome secondary to HIV. J Clin Images Med Case Rep. 2025; 6(2): 3490
Background
Hemophagocytic Lymphohistiocytosis (HLH) is an aggressive and life-threatening syndrome characterized by excessive immune activation. It is marked by abnormal activation of macrophages and T cells, leading to a cytokine storm with high morbidity and mortality [1]. HLH is classically divided into two types: 1) primary and 2) secondary. Secondary HLH can be associated with autoimmune diseases, infectious diseases, malignancy, immunosuppression, transplantation, Human Immunodeficiency Virus (HIV), and metabolic diseases. HLH carries a high risk of progression to Multi-Organ Dysfunction Syndrome (MODS), including Acute Kidney Injury (AKI). The uncontrolled activation of T lymphocytes and macrophages, combined with impaired cytotoxic function of NK cells, results in massive cytokine release and a hyperinflammatory phenotype. This is the target for treatment, which aims to suppress the hyperinflammatory state by targeting activated CD8+ T lymphocytes and macrophages [2].
HLH usually presents as an acute or subacute febrile illness associated with multiple organ involvement. Diagnosis is based on a compatible clinical presentation with elevated inflammatory markers. HLH must be distinguished from other multisystem illnesses that involve fever, liver failure, and/or neurologic symptoms. Early identification is critical since delayed diagnosis remains a major barrier to successful treatment and outcomes in individuals with HLH. Blood purification techniques, such as hemoadsorption, can help mitigate the inflammatory process with a rapidly relevant, nonselective effect on the cytokine storm [3]. Cytokine adsorption using the CytoSorb absorber has been proposed in various clinical settings, including hyperinflammatory syndromes [4].
Data primarily demonstrate the effectiveness of hemoadsorption in the context of sepsis, showing it to be an effective treatment compared to CVVHDF for the removal of inflammatory cytokines [5]. The use of CytoSorb for cytokine adsorption has been explored in various clinical contexts, including hyperinflammatory syndromes [6].
Methods
A 37-year-old male arrived at the ER with 3 days of abdominal pain, jaundice, nausea, and vomiting. His laboratory results upon admission are shown in Table 1. He had a negative HIV test 6 months prior to admission. Physical examination revealed no signs of neurological compromise, though he was tachypneic and in respiratory distress. He exhibited jaundice, a temperature of 38°C, a mean arterial pressure (MAP) of 60 mmHg, an oxygen saturation (SatO2) of 92%, and no lymphadenopathy. Abdominal examination revealed painful hepatosplenomegaly and ascites. After 48 hours, the patient developed neurological symptoms, and Multi-Organ Dysfunction Syndrome (MODS), including kidney, liver, lung, and hematological involvement, became evident. HIV testing by molecular biology, CD4 viral load, and Epstein-Barr Virus testing were performed, as shown in Table 2.
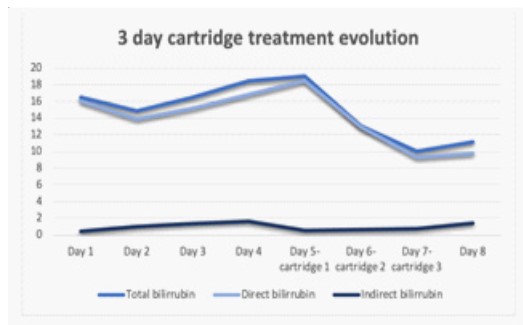
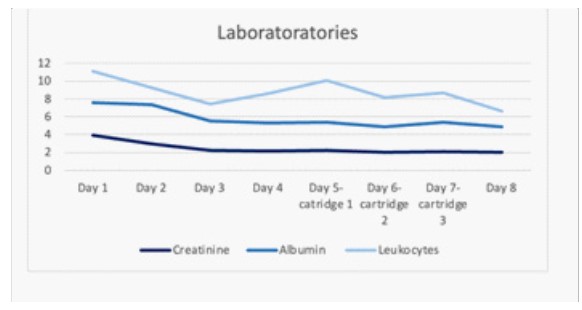
Antiretroviral therapy, antibiotics, and Continuous Renal Replacement Therapy (CRRT) were initiated with the following prescription: HDFVVC at 30 ml/kg/hr, with no anticoagulation, using an oXiris® membrane. The initial response was poor, and the patient’s clinical condition deteriorated. On day 4, hemoperfusion with CytoSorb was started to attempt to improve the cytokine storm and hyperbilirubinemia. A decrease in bilirubin levels, shown in Figure 1, was observed, as well as a reduction in IL-6 levels from 114.20 pg/mL to 38.56 pg/mL.As well as a decrease in another parameter shown in Figure 2, three sessions of hemoperfusion were performed, each lasting 24 hours. On day 6, the patient developed severe refractory respiratory acidosis, which required invasive mechanical ventilation (IMV). HLH was suspected, but bone marrow aspiration for diagnostic confirmation could not be performed due to the patient’s hemodynamic instability. An H-score diagnostic criterion was applied, indicating an 88% probability of HLH. Rituximab and corticosteroids were started. Unfortunately, despite treatment, the patient’s clinical condition continued to deteriorate rapidly, and he passed away the following day.
Results
Inflammatory cytokines, including IL-6, as well as bilirubin, leukocyte count, and creatinine levels, decreased after the use of hemoperfusion in a patient with multi-organ failure secondary to HLH, which developed due to a recent HIV infection. These observations suggest that an adequate response in terms of inflammatory cytokines following CytoSorb treatment could provide the patient with additional time to initiate the necessary therapeutic interventions for the underling disease.
Additionally, the mortality outcome in this case did not differ from the results described in previous studies, which indicate that although hemoperfusion cartridges can help mitigate the hyperinflammatory state, they do not directly impact mortality. Further studies are needed to reevaluate the relationship between hemoperfusion and mortality outcomes.
Relevant laboratory results:
Table 1: Admission laboratories.
| Laboratory test | Patient result |
|---|---|
| Creatinine, mg/dl | 3.69 (H) |
| Total bilirubin, mg/dl | 16.12 (H) |
| Bilirubin direct, mg/dl | 15.08 (H) |
| Bilirubin indirect, mg/dl | 1 (H) |
| AST, U/l | 125 (H) |
| ALT, U/l | 89 (H) |
| LDH, UI/L | 1026 (H) |
| Amylase, U/L | 713 (H) |
| Lipase, U/L | 2388 (H) |
| Lactate, mmol/L | 11.3 (H) |
| Hemoglobin, g/dL | 12 (L) |
| WBC count | 3.5 (L) |
| Lymphocytes | 0.65 (L) |
| Platelets | 43 (L) |
| Ammonia, ug/dL | 255 (H) |
Table 2: Viral loads.
| Laboratory test | Patient result |
|---|---|
| HIV, copies/ml | 590,000 (H) |
| CD4+ count, cells/uL | 38.19 (H) |
| EBV, copies/ml | 3,150,000 (H) |
Discussion
Cytokine adsorption with CytoSorb, as proposed in clinical settings such as sepsis, ARDS, hyperinflammatory syndromes, and cardiac surgery, serves as a bridge for the initiation of required therapy. The aim of this study was to provide clinical evidence of the reduction in inflammatory cytokines in an atypical presentation of HIV with HLH, where the need for antibiotics to address superinfections, antiretroviral therapy, and multiorgan support was delayed due to the patient’s hyperinflammatory state.
Pro-inflammatory cytokines lead to vasodilation, capillary leakage, and coagulopathy, while anti-inflammatory cytokines can cause relative immunosuppression, increasing susceptibility to secondary nosocomial infections. The uncontrolled release of both types of cytokines can result in multiple organ failure, as seen in our patient. For this reason, controlling cytokines serves as a bridge to initiate the necessary therapy for treating the underlying disease.
Conclusion
We present the case of an atypical presentation of acquired HIV infection, characterized by rapid progression and clinical deterioration, leading to the development of HLH and subsequent MODS. This required extracorporeal support, including invasive mechanical ventilation (IMV), continuous renal replacement therapy (CRRT), and hemoperfusion. Certain extracorporeal blood purification techniques can reduce excess inflammatory mediators and remove bilirubin. The use of the hemoperfusion cartridge, which helps reduce the cytokine storm and bilirubin—as demonstrated in this case—could improve certain clinical parameters and serve as a bridge to specific HLH treatments, such as the HLH-94 protocol, though it does not have a direct impact on survival. This case highlights the possibility of MODS as the initial presentation of acquired HIV and the potential use of CytoSorb for cytokine control.
Declarations
Acknowledgement: We thank the Hospital Christus Muguerza Alta Especialidad and the biostatistics department for their assistance with the clinical data files.
Conflict of interest: The authors have no conflicts of interest to declare.
Author contributions: All authors fulfill the ICMJE Criteria for Authorship based on four main criteria: contribution to the concept and design of the work, draft important intellectual content, revise the final version, and agree to be accountable. As for Lilia María Rizo Topete, the corresponding author, made a substantial contribution to the acquisition of data, as well as actively participated in the final approval of the version and critically revised it. Juan Pablo Gómez Villarreal actively participated in the acquisition of data and drafted the manuscript. He also agreed to ensure that the manuscript was appropriately investigated. Ricardo Garza Treviño was involved in drafting the manuscript, critically revising it, and adding the required information to create adequate intellectual content. Rolando Clauré del Granado contributed to the final revision with language proof revision. Paola Borbolla Flores made a substantial contribution to the conception, design, and data acquisition. She also made final contributions before the final approved version was revised by the corresponding author.
References
- Campo M, Berliner N. Hemophagocytic lymphohistiocytosis in adults. Hematology/Oncology Clinics of North America. 2015; 29: 915-925.
- Machaczka M. Limfohistiocytoza hemofagocytarna-współczesny problem medyczny [Hemophagocytic lymphohistiocytosis--a contemporary medical problem]. Pol Merkur Lekarski. 2012; 32: 59-63.
- Bottari G, Murciano M, Merli P, Bracaglia C, Guzzo I, Stoppa F, et al. Hemoperfusion with CytoSorb to Manage Multiorgan Dysfunction in the Spectrum of Hemophagocytic Lymphohistiocytosis Syndrome in Critically Ill Children. Blood Purif. 2022; 51: 417-424.
- Becker S, Lang H, Vollmer Barbosa C, et al. Efficacy of CytoSorb®: a systematic review and meta- analysis. Crit Care. 2023; 27: 215.
- Ceruti S, Glotta A, Adamson H, Mauri R, Molnar Z. Hemoadsorption Treatment with CytoSorb® in Probable Hemophagocytic Lymphohistiocytosis: A Role as Adjunctive Therapy? Case Rep Hematol. 2021; 2021: 5539126.
- Becker S, Lang H, Vollmer Barbosa C, et al. Efficacy of CytoSorb®: a systematic review and meta- analysis. Crit Care. 2023; 27: 215.