
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A case of rhabdomyolysis accompanied by reversible mitral valve prolapse and regurgitation
Toru Maruyama*; Hiroaki Nishikata; Takako Nakazono; Michiaki Kubo; Hideyuki Nomura
Haradoi Hospital, Fukuoka 813 8588, Japan
*Corresponding Author : Toru Maruyama
Haradoi Hospital, Aoba 6 40 8, Higashi-ku, Fukuoka
813 8588, Japan.
Tel: +81 92 691 3881;
Email: tmaruyama@haradoi-hospital.com
Received : Feb 01, 2025
Accepted : Feb 24, 2025
Published : Mar 03, 2025
Archived : www.jcimcr.org
Copyright : © Maruyama T (2025).
Abstract
Rhabdomyolysis is caused by skeletal muscle destruction, potentially lethal, and requiring correct diagnosis and appropriate management to prevent acute renal failure and subsequent multiorgan failure. Although cardiomyopathy leading to heart failure and arrhythmia are the main cardiac complications of symptomatic inherited skeletal myopathies observed in lysosomal storage diseases and progressive muscular dystrophies, cardiac involvement of rhabdomyolysis is rare. Herein, we report a case of rhabdomyolysis induced by psychotic drugs and accompanied by mitral valve prolapse and functional regurgitation, which was reversible during the clinical course of rhabdomyolytic recovery. This case reconfirmed the pathogenic and pathophysiologic associations of skeletal muscles disorders with cardiac muscle dysfunction.
Keywords: Rhabdomyolysis; Mitral valve prolapse; Mitral regurgitation.
Citation: Maruyama T, Nishikata H, Nakazono T, Kubo M, Nomura H. A case of rhabdomyolysis accompanied by reversible mitral valve prolapse and regurgitation. J Clin Images Med Case Rep. 2025; 6(3): 3491.
Introduction
Both skeletal and cardiac muscles are striated muscles, and these two types of muscles share the same fate in terms of exercise adaptation, withering by senile frailty, and some inherited systemic or musculoskeletal disorders involving myocardium such as lysosomal storage diseases [1-3] and many kinds of progressive muscular dystrophies [4-6]. Rhabdomyolysis is based on the skeletal muscle injury by many etiologies such as trauma, infection, drugs, toxins, electrolyte imbalance, metabolic disorder, and muscular exhaustion [7]. This clinical entity is characterized by skeletal muscle degradation, leakage of intramuscular contents, and diagnosed by blood chemistry showing elevation of myogenic enzyme activities [8]. Herein, we present a case of psychotics-induced rhabdomyolysis accompanied by severe but reversible mitral valve prolapse and regurgitation.
Case presentation
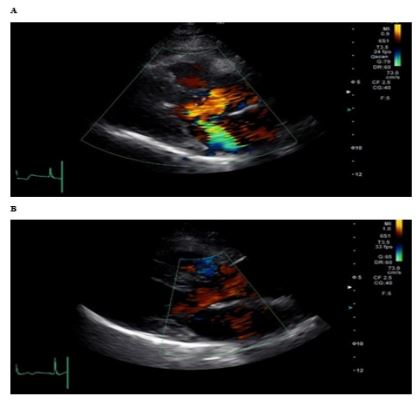
A 57-year-old lady visited the emergency department of our hospital complaining muscle weakness and dark urine. Her lower leg muscles were shivering, restless and weak. She wanted to keep standing because it was hard to stand up again after sitting. She had no history of cardiac diseases causing heart murmurs, no recent experience of traumatic accident or invasive medical procedure. She was a non-smoker and a non-drinker, but complaining of headache, and prescribed regularly with psychotic drugs (amitriptyline 30 mg per day, etizolam 1.00 mg per day, and lorazepam 0.5 mg per day) by a psychiatric doctor in the outpatient clinic. A week before the admission, domperidone (30 mg), sulpiride (100 mg) and biperiden (1 mg) were added, and she complained of muscle weakness and pain. Statin or antiplatelet was not prescribed. Laboratory data showed a marked elevation of CPK, AST, ALT, and LDH (Table 1). She admitted to our hospital immediately under the diagnosis of rhabdomyolysis accompanied by tea-colored urine. After admission, she hesitated to lie down because of the involuntary muscular shivering due to weakness. She was anorexic and intravenous drip infusion was started immediately for intravascular fluid management, nutrition and renal protection. All psychotic drugs were ceased. Auscultation revealed evident holosystolic murmur (IV/VI°) not only in parasternal and apical region but also in the back. Ultrasound cardiography (UCG) demonstrated anterior mitral valve prolapse and severe mitral regurgitation. Regurgitant flow directed to the left atrial posterior wall (Figure 1A). Daily drip infusion with 1,000-1,500 mL of crystalloid fluid was continued for six days, and enzyme levels were normalized gradually (Table 1). Eight days before discharge, urine color was straw-yellow, and we attempted UCG again since heart murmur disappeared. It was confirmed that severe mitral prolapse and regurgitation disappeared on UCG (Figure 1B). Her physical activity was elevated after myalgia was faded, laboratory data were almost normalized, and she discharged one month after admission.
Table 1: Laboratory data during the clinical course.
| Days | 0 | 1 | 4 | 6 | 12 | 15 | 22 | 27 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Event | UCG | UCG | ||||||||
| Drip (mL) | 1,500 | 1,500 | 1,000 | 1,000 | - | - | ||||
| Blood chemistry | (normal range: unit) | |||||||||
| CPK | 41-153 U/L | - | 32,308 | 23,548 | 2,657 | 999 | 196 | 105 | 50 | 37 |
| AST | 13-30 U/L | 42 | 745 | 551 | 107 | 42 | 21 | 16 | 16 | 14 |
| ALT | 7-30 U/L | 66 | 300 | 282 | 157 | 106 | 44 | 32 | 23 | 18 |
| ALP | 38-113 U/L | - | 118 | 97 | 80 | 82 | 95 | 108 | 131 | 121 |
| LDH | 124-222 U/L | - | 1,318 | 1,249 | 792 | 614 | 359 | 274 | 206 | 171 |
| g-GTP | 9-32 U/L | 375 | 185 | 164 | 110 | 100 | 105 | 114 | 130 | 124 |
| BUN | 8-20 mg/dL | 11 | 21.7 | 14.4 | 7.4 | 8.1 | 9.9 | 10.2 | 5.9 | 6.8 |
| Creatinine | 0.46-0.79 mg/dL | 0.64 | 1.08 | 0.68 | 0.6 | 0.58 | 0.66 | 0.72 | 0.66 | 0.69 |
| eGFR | > 60 mL/min/1.73m2 | 70.8 | 39.1 | 64.9 | 74.4 | 77.2 | 67 | 61 | 67 | 63.9 |
| Total protein | 6.6-8.1 g/dL | - | 8 | 6.8 | 5.8 | - | - | - | 7.3 | 7.2 |
| Albumin | 4.1-5.1 g/dL | - | 5.1 | 4.3 | 3.7 | - | - | - | 4.7 | 4.6 |
| Na | 138-145 mM/L | 138 | 134 | 135 | 144 | 144 | 144 | 143 | 142 | 142 |
| K | 3.6-4.8 mM/L | 3.8 | 3.8 | 3.4 | 3.1 | 3.2 | 3.4 | 3.4 | 3.5 | 3.5 |
| Uric acid | 2.6-5.5 mg/dL | - | 4.7 | 3.6 | 2.6 | 2.7 | 2.5 | 2.9 | 3.2 | 3.4 |
| Cholesterol | 142-248 mg/dL | - | 238 | - | - | - | - | - | 213 | 212 |
| Triglyceride | 30-117 mg/dL | - | 104 | - | - | - | - | - | 88 | 130 |
| Hemoglobin | 11.6-14.8 g/dL | 12.3 | 14.6 | 12.5 | 11.3 | 11 | 11.5 | 11.8 | 12.7 | 12.7 |
| CRP | <0.14 mg/dL | 0.24 | 1.26 | 0.07 | 0.05 | 0.05 | 0.05 | 0.05 | ||
| Urine chemistry | ||||||||||
| Color | tea-colored | straw-yellow | straw-yellow | |||||||
| Protein | ++ | - | - | |||||||
| Cloudy | + | - | - | |||||||
| Protein/g•cr | ++ | N | N | |||||||
| Albumin/g•cr | + | N | N | |||||||
| Creatinine | 200 | 100 | 100 | |||||||
| Sugar | - | - | - | |||||||
| Specific gravity | 1.02 | 1.01 | 1.01 | |||||||
| pH | 4.8-7.5 | 6.5 | 7 | 6.5 | ||||||
| Urobilinogen | N | N | N | |||||||
| Keton | - | - | - | |||||||
| WBC | +++ | - | - | |||||||
| Occult blood | +++ | - | - |
Alteration of laboratory data were indicated during the clinical course. Day 0 indicates the day of admission. Drip infusion was performed to prevent hypovolemia and renal failure. Marked elevation of myogenic leakage enzymes (CPK, AST, ALT, and LDH), mild elevation in CRP, and transient renal dysfunction (decline in eGFR) were noted in blood chemistry. Urine color and proteinuria in urine dipstick test indicate myoglobinuria, whereas numerous blood cells appearing in urine microscopic examination suspect transient acute glomerular or tubular damage [20,21]. Intensive fluid administration was performed until 6 days after admission. Laboratory data demonstrated on the top left column was obtained 4 years before admission, whereas those on the top right column (27 days) was obtained 3 days before discharge.
Discussion
The case presented here had the history of prescription with multiple psychotics, and the onset of muscular symptom coincided well with the up titration of these psychotics. Mild elevation in CRP relative to marked elevation of myogenic enzymes indicates that inflammatory myositis is unlikely in this case. She had no episodes of trauma or invasive medical procedure. Laboratory data restored, and symptoms improved after the withdrawal of all the psychotics and starting intensive fluid therapy, implying that drug-induced rhabdomyolysis is most likely. Clinical spectrum of rhabdomyolysis is variable ranging from asymptomatic elevation in CPK to acute tubular necrosis due to myoglobinuria. Rhabdomyolysis is sometimes fatal because of acute renal failure leading to multiorgan failure [7,8]. Therefore, early diagnosis and prompt management are required for clinicians. Although the patient described here was managed successfully, incidental cardiac event was unanticipated.
Cardiac involvement of rhabdomyolysis is relatively rare. Skeletal myocytes destruction releases toxic intracellular components including potassium into the circulation, which induces hyperkalemia [9,10]. Furthermore, ionized calcium deposits onto the necrotic muscles, which causes hypocalcemia [11]. Therefore, cardiac arrhythmia based on the rhabdomyolysisinduced electrolytes imbalance is one of the main cardiac complications [9,10]. Furthermore, Ambra et al reported a case of rhabdomyolysis and muscular abscess accompanied by infective endocarditis [12]. The exact mechanism of prolapsing and subsequent regurgitation of mitral leaflets are unknown in this case. Functional mitral regurgitation (FMR) is divided into two types, i.e., FMR secondary to ventricular remodeling and FMR due to atrial enlargement [13]. Left atrial volume remained normal and no atrial fibrillation was recorded during hospitalization, whereas normal left ventricular contractility suggests that non-ischemic cardiomyopathy was unlikely in this case (Figure 1). Furthermore, atrial or ventricular remodeling is unlikely to reverse within a month. Considering no atrial or ventricular causes of reversible FMR, rhabdomyolysis-related papillary muscle dysfunction may have induced tethering leading to the coaptation failure of intact mitral leaflets. Because papillary muscles are susceptible to transient ischemia [14], inflammation [15] or metabolic derangement [16], and dysfunctional papillary muscles are reported to be a new substrate of FMR [17,18]. More sophisticated imaging modalities such as papillary muscle longitudinal strain UCG or stress cardiac magnetic resonance may have clarified the exact mechanisms responsible for the mitral leaflet coaptation failure leading to the reversible FMR [18,19].
Conclusion
The case presented here indicates clearly the cardiac involvement of rhabdomyolysis in terms of simultaneous clinical course, i.e., mitral prolapse and regurgitation was detected immediately after the onset of rhabdomyolysis, and such cardiac involvement was fading according to the recovery of muscular weakness and declining the myogenic enzyme activities. Reversible cardiac involvement in drug-induced rhabdomyolysis confirmed in the present case implies the metabolic, energetic, and pathogenic linkage between the skeletal and cardiac muscles.
Declarations
Funding sources: All authors have no funding sources on this article.
Conflict of interest statement: All authors have no conflict of interest with respect to this article.
Acknowledgements: All authors acknowledge the nursing, laboratory and rehabilitation staffs taking care of the patient corresponding to the presented case.
Author contributions: TM was responsible for conceptualization, data collection, and original draft writing. HN (the second author) was responsible for taking care of this case in the outpatient clinic as a specialist of psychosomatic medicine. MK was responsible for taking care of this case in the emergency department. TN was responsible for taking care of this case during hospitalization. HN (the last author) has supervised the team collaboration as a president of our hospital. All coauthors have reviewed the manuscript and approved the final version submission and taking public responsibility with respect to this article.
Data availability statement: The data supporting the findings of this case report are available from the corresponding author upon reasonable request (tmaruyama@haradoi-hospital. com).
References
- Gümüş E, Özen H. Glycogen storage diseases: an update. World J Gastroenterol. 2023; 29 (25): 3932-63.
- Sestito S, Parisi F, Tallarico V, Tarsitano F, Roppa K, et al. Cardiac involvement in lysosomal storage diseases. J Biol Regul Homeost Agents. 2020; 34 (4 Suppl. 2): 107-19.
- Nair V, Belanger EC, Veinot JP. Lysosomal storage disorders affecting the heart: a review. Cardiovasc Pathol. 2019; 39: 12-24.
- Mavrogeni SI, Markousis-Mavrogenis G, Papavasiliou A, Papadopoulos G, Kolovou G. Cardiac involvement in Duchenne muscular dystrophy and related dystrophinopathies. Methods Mol Biol. 2018; 1687: 31-42.
- Fayssoil A, Abasse S, Silverston K. Cardiac involvement classification and therapeutic management in patients with Duchenne muscular dystrophy. J Neuromuscul Dis. 2017; 4 (1): 17-23.
- Silvestri NJ, Ismail H, Zimetbaum P, Raynor EM. Cardiac involvement in the muscular dystrophies. Muscle Nerve. 2018; 57 (5): 707-15.
- Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: Rhabdomyolysis - an overview for clinicians. Crit Care. 2005; 9 (2): 158-69.
- Sever MS. Rhabdomyolysis. Acta Clin Belg. 2007; 62 (Suppl 2): 375-9.
- Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med. 2009; 67 (9): 272-83.
- Sauret JM, Marinides G, Wang GK. Rhabdomyolysis. Am Fam Physician. 2002; 65 (5): 907-12.
- Davis AM. Hypocalcemia in rhabdomyolysis. JAMA. 1987; 257 (5): 626. Erratum in: JAMA 1987; 258 (14): 1894.
- Ambra N, Palol A, Moidy MJ, Kordi A, Almughalles S, et al. Infective endocarditis presenting as rhabdomyolysis and muscle abscess: a case report. Cureus. 2023; 15 (11): e49682.
- Schmitto JD, Lee LS, Mokashi SA, Bolman RM 3rd, Cohn LH, et al. Functional mitral regurgitation. Cardiol Rev. 2010; 18 (6): 285- 91.
- Cheng TO. Papillary muscle dysfunction due to coronary artery spasm. J Cardiol. 2006; 47 (5): 270-1.
- Tomaru T. The multifactorial etiology of mitral valve prolapse, a new entity of postinflammatory mitral valve prolapse. Herz. 1988; 13 (5): 271-6.
- Karlsson J, Sylvén C, Jansson E, Böök K, Muratsu K, et al. Coenzyme Q10 and key enzyme activities in papillary muscle related to left ventricle function in mitral valve disease. Mol Cell Biochem. 1988; 84 (1): 59-64.
- Sanyal SK, Johnson WW, Dische MR, Pitner SE, Beard C. Dystrophic degeneration of papillary muscle and ventricular myocardium. A basis for mitral valve prolapse in Duchenne’s muscular dystrophy. Circulation. 1980; 62 (2): 430-8.
- Kochav JD, Kim J, Judd R, Kim HW, Klem I, et al. Ischemia-mediated dysfunction in subpapillary myocardium as a marker of functional mitral regurgitation. JACC Cardiovasc Imaging. 2021; 14 (4): 826-39.
- Kılıcgedik A, Kahveci G, Gurbuz AS, Karabay CY, Guler A, et al. Papillary muscle free strain in patients with severe degenerative and functional mitral regurgitation. Arq Bras Cardiol. 2017; 108 (4): 339-46.
- Young SE, Miller MA, Docherty M. Urine dipstick testing to rule out rhabdomyolysis in patients with suspected heat injury. Am J Emerg Med. 2009; 27 (7): 875-7.
- Amini M, Sharifi A, Najafi I, Eghtesadi-Araghi P, Rasouli MR. Role of dipstick in detection of haeme pigment due to rhabdomyolysis in victims of Bam earthquake. East Mediterr Health J. 2010; 16 (9): 977-81.