
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Heterotopic gastric mucosa in the rectum during follow-up for colon cancer: A rare case and a systematic review
Andrea Bottari1*; Giuseppina Colasanto1 ; Simone Buccianti1 ; Giulia Cavallina1 ; Veronica Matteoni2 ; Rossella Occhini2 ; Alessandro Tedone1 ; Giorgio Cangioni1 ; Francesco Renzi1
1General and Emergency Surgery Department, Valdarno Hospital, Arezzo, Italy
2Pathological Anatomy Department, S. Donato Hospital, Arezzo, Italy
*Corresponding Author : Andrea Bottari
General and Emergency Surgery Department,
Valdarno Hospital, Piazza del Volontariato 2, 52025,
Arezzo, Italy.
Email: andrea.bottari@uslsudest.toscana.it
Received : Jan 27, 2025
Accepted : Feb 24, 2025
Published : Mar 03, 2025
Archived : www.jcimcr.org
Copyright : © Bottari A (2025).
Abstract
Introduction: Heterotopic mucosa is defined as morphologically normal tissue found in a different anatomical site and separated from its organ of origin. Heterotopic Gastric Mucosa (HGM) is a rare finding and it’s the most frequent type of heterotopia. Heterotopic Gastric Mucosa (HGM) affects mainly the esophagus and rarely the rectum, appearing as a raised lesion. The main differential diagnosis is with cancer lesions.
Presentation of the case: A 53-year-old woman was admitted to our institution for an endoscopic follow-up after sigmoid cancer. Control revealed a flat lesion of the rectum, Paris classification type IIa+IIc, starting from the dentate line for approximately 20 mm up to the anal canal, 15 mm in diameter, with a smooth surface and visible edges, on which five biopsies were performed (Figures 1 and 2). The patient denied any history of blood in the stool, anal fissures, or fistulas. Pathological histology suggested HGM-related findings in the rectal mucosa.
Results and discussion: Given the ultra-low position in the anal canal, the patient where referred to surgical excision with direct closure of the mucosal breach, under local anesthesia. The postoperative course was uneventful with complete functional recovery.
Conclusion: HGM is usually associated with gastrointestinal tract abnormalities. The coexistence of HGM within diverticula often leads to an increased incidence of bleeding and perforation. The literature revealed that HGM can be carcinogenic; a long-standing rectal HGM may lead to an increased cancer risk and should be followed endoscopically or resected. Conventional Endoscopic Mucosal Resection (EMR) is indicated for lesions up to 20 mm, otherwise, the risk of local recurrence increases significantly; Endoscopic Submucosal Dissection (ESD) allows removal of lesions exceeding 20 mm; surgery is more invasive and exposes the patient to greater intra- and post-operative risks. In the present case, the lesion reached the dentate line. Treatment with EMR would have been difficult for the size and would have risked not including it en-bloc, inhibiting the margins evaluation. ESD could have effectively addressed these limitations, but given the proximity of the lesion to the dentate line, it was technically very difficult to proceed with an ESD safely, so we performed a surgical transanal excision.
Keywords: Gastric ectopia; Rectal surgery; Endoscopy; General surgery.
Abbreviations: HGM: Heterotopic Gastric Mucosa; EMR: Endoscopic Mucosal Resection; ESD: Endoscopic Submucosal Resection.
Citation: Bottari A, Colasanto G, Buccianti S, Cavallina G, Matteoni V et al. Heterotopic gastric mucosa in the rectum during follow-up for colon cancer: A rare case and a systematic review. J Clin Images Med Case Rep. 2025; 6(3): 3492.
Background
Heterotopic mucosa, the most frequent being Heterotopic Gastric Mucosa (HGM), is defined as morphologically normal tissue found in a different anatomical site, separated from its organ of origin. HGM is categorized into congenital (heteroplasia) or acquired (metaplasia). In the case of acquired HGM, it appears to result from incorrect positioning of stem cells during organogenesis or faulty differentiation of pluripotent cells in damaged epithelium.
This entity is predominantly found in the esophagus, presenting as a raised lesion. HGM is more frequently observed in the upper esophagus (15%-30% of cases), in the duodenum, and in the small intestine (0.1-10%). However, its occurrence in the rectum is extremely rare. In the rectum, HGM appears endoscopically as an elevated, flat, or superficial lesion with variable size and morphology. Biopsy is crucial for establishing the main differential diagnosis, particularly with neoplasms. Recent trends show increased interest in endoscopic treatment over the previously preferred surgical procedure [1,2].
Materials and methods
To conduct a literature review on rectal HGM from the initial description in 1939 [3] to July 2023, we employed Pubmed, MEDLINE, EMBASE, and Google Scholar. The search encompassed relevant papers using keywords such as “heterotopic gastric mucosa,” “gastric heterotopic,” and “rectum” without language restrictions. In instances where multiple publications originated from the same author, each case was distinguished by demographic characteristics to prevent duplication.
For patients with HGM, we extracted various data points, including age and sex, size, morphology, location, histological features, clinical symptoms, presence of associated deformities/complications, treatment modality, recurrence rate, and symptom relief rate. Following the Paris classification [4], HGM was morphologically categorized into elevated lesions (0-I), flat lesions (0-II), and depressed lesions (0-III). Type 0-I was further classified into tipped (0-Ip) and untipped (0-Is), while Type 0-II had three subtypes (0-IIa, 0-IIb, and 0-IIc) corresponding to slightly elevated, flat, and slightly depressed lesions, respectively. The distinction between type 0-I and type 0-IIa was based on the height of augmentation, up to 2.5 mm (thickness of biopsy forceps closing).
The boundary between type 0-III and type 0-IIc was determined by the depth of depression, up to 1.2 mm (thickness of individual forceps of biopsy forceps opening). Lesions with both slight elevation and slight depression were classified as 0-IIc + IIa and 0-IIa + IIc types based on the elevation/depression ratio. Additionally, lesions with a combination of depression and slight depression were categorized as III + IIc and 0-IIc + III types, depending on the ratio of depression/slight depression.
Results
Since the initial description by Ewell and Jackson in 1939 [3], a total of 48 cases of rectal HGM have been reported, encompassing the one case presented in this study. Nine studies were excluded due to duplication (3 cases) or non-rectal HGM cases with incomplete information (6 cases). The evaluation of the 48 cases is detailed in (Table 1) [2]. The median age of the patients was 25 years, ranging from 1 day after birth to 69 years, with 18 minors (<18 years) and 29 adults (≥18 years). Males constituted 53.2% of the cases.
The rectum was categorized into three segments, with 29 cases (60.4%) located in the low rectum, 8 cases (14.6%) in the middle rectum, and 12 cases (25%) in the proximal rectum. The mean lesion size was 26.67±13.04 mm, ranging from 1 mm to 60 mm. The morphology of HGM was classified according to the Paris classification [4]. Flat lesions (type 0-II) constituted 39.5% of cases, with subtypes including slightly elevated lesions (type 0-IIa), flat lesions without elevation (type 0-IIb), and superficial elevation with depression (type 0-IIa-IIc). Polypoid elevations (0-Is, 0-Ip, and 0-Isp types) accounted for 43.7% of cases, while deep depressions (0-III types) were observed in 8.3% of cases. The presence of diverticula or repetitive digestive tract malformations was noted in 23.9% of cases, with other complications, including rectal mucosal ulcers and rectal perforation, observed in 21.7%.
The histological analysis of 45 cases (93.75%) reported fundic gland mucosa as the most common type (81.2%). Mixed mucosa of the pyloric and fundic glands, mucosa of the pyloric gland, and mucosa of the cardia gland were observed in a smaller proportion of cases. Additionally, there were rare instances of intestinal metaplasia, pancreatic adenoma with low-grade intraepithelial neoplasia, and high-grade intraepithelial neoplasia. Helicobacter pylori (HP) detection by Giemsa or Warthin Starry staining revealed positive results in 18.6% of cases.
Clinical symptoms predominantly included abnormal bowel movements, abdominal pain, blood in the stool, and anal pain. Among the patients, 23.9% were asymptomatic, and 10.8% had abdominal symptoms. Anorectal-related symptoms were prevalent in 59.7% of cases, with anal pain and blood in the stool more common in children (<18 years) than adults (72.2% vs. 37.9%, respectively).
Of the cases, 72.9% underwent treatment, with 45,7% undergoing surgical resections, 34.2% undergoing Endoscopic Mucosal Resection (EMR), and 14.2% undergoing Endoscopic Submucosal Dissection (ESD). Surgical treatment was more common in minors (44.4%) than in adults (23.5%). Pharmacological treatment, including H2 receptor antagonists, proton pump inhibitors, bismuth, and antibiotic therapy, and/or eradication of HP, was administered in 42.6% of cases. ESD-treated cases showed no significant bleeding or perforation complications, and conservative treatment proved effective in symptom control and ulcer healing.
After HGM resection and a median follow-up of 21 months (range 1-84), no recurrence was observed in any case following CT scans and colonoscopy
Case report
A 53-year-old female was admitted to the hospital for an endoscopic evaluation following rectal bleeding after a recent left hemicolectomy for a cancerous polyp in the sigmoid colon. The examination revealed a flat lesion in the rectum extending to the dentate line, classified as 0-IIa according to the Paris Classification, approximately 35 mm in size, with a smooth surface and well-defined borders. Biopsies of the lesion were performed, which confirmed the presence of ectopic gastric mucosa in the rectum. The patient underwent transanal surgical excision of the lesion. The postoperative course was uneventful, and the patient was discharged on the same day. Postoperative histopathological analysis confirmed the immunophenotypic findings of gastric heterotopia in the rectal mucosa, which was completely excised. Therefore, a diagnosis of HGM was established. At the 1-month follow-up, the patient had recovered well and reported no further blood in the stool or any other symptoms.
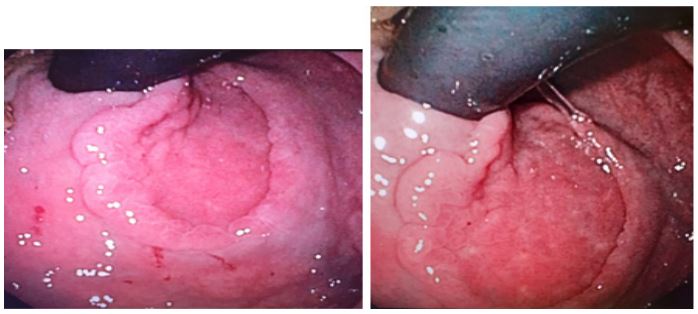
Table 1: HGM analyzed cases.
| Age (yr) | Sex | Malformation | Location | Morphology | Size (mm) | Complication | Mucosa type | Treatment |
|---|---|---|---|---|---|---|---|---|
| 0 | F | Multiple | Proximal | 0-Ib | No | Mixed | Med | |
| 1 | F | No | Low | 0-Is | 25 | No | Oxyntic | Surgery |
| 2 | F | No | Low | 0-IIa | 30 | No | Surgery | |
| 3 | F | No | Low | 0-IIa + IIc | 30 | Bleeding | Oxyntic | ESD |
| 3 | M | No | Low | 0-I | No | Oxyntic | Surgery | |
| 4 | M | No | Low | 0-IIa + IIc | 50 | Ulcer | Surgery | |
| 4 | F | RD | Low | 0-II | 35 | No | Oxyntic | Med |
| 4 | M | No | Proximal | 0-IIa | 40 | Bleeding | Oxyntic | EMR |
| 4 | M | No | Low | 0-Is | 15 | Ulcer | Oxyntic | EMR |
| 5 | M | No | Low | 0-Is | 10 | No | Oxyntic | Surgery |
| 5 | F | No | Low | 0-IIa + IIc | 40 | No | Oxyntic | EMR |
| 5 | F | RD | Proximal | 0-III | 20 | Perforation | Oxyntic | Med |
| 6 | M | No | Low | 0-I | 1 | Ulcer | Oxyntic | Med |
| 7 | M | No | Middle | 0-Is | 15 | No | Oxyntic | EMR |
| 10 | M | RD | Proximal | 0-IIa | 20 | Ulcer | Oxyntic | Surgery |
| 10 | M | No | Proximal | 0-Is | 30 | Ulcer | Oxyntic | Surgery |
| 14 | F | RD | Low | 0-IIa | 50 | No | Oxyntic | ESD |
| 16 | M | No | Low | 0-I | 30 | Ulcer | Oxyntic | Surgery |
| 19 | F | Multiple | Low | 0-Ip | Perforation | Oxyntic | Med | |
| 20 | M | No | Proximal | 0-III | 15 | Ulcer | Oxyntic | EMR |
| 22 | M | No | Low | 0-II | 50 | No | Oxyntic | Med |
| 22 | M | No | Middle | 0-IIa + IIc | 40 | No | Oxyntic | Surgery |
| 25 | M | No | Middle | 0-IIa | 40 | Bleeding | Oxyntic | EMR |
| 28 | M | RD | Middle | 0-Is | 60 | No | Oxyntic | Surgery |
| 28 | F | No | Low | 0-I | No | Mixed | Med | |
| 28 | F | No | Low | 0-IIb | 20 | Bleeding | Oxyntic | ESD |
| 31 | M | No | Middle | 0-IIa | 20 | No | Oxyntic | Med |
| 33 | M | No | Low | 0-Ip | 18 | Anal pain | Oxyntic | EMR |
| 34 | M | No | Low | 0-Is | 25 | No | Oxyntic | EMR |
| 35 | F | RD | Middle | 0-IIb | 10 | No | Oxyntic | Ablation |
| 36 | F | No | Low | 0-Is | 25 | No | Oxyntic | EMR |
| 45 | M | No | Proximal | 0-Ip | 20 | No | Mixed | Surgery |
| 45 | M | Diverticula | Low | 0-IIa + III | 30 | Bleeding | Oxyntic | ESD |
| 46 | F | No | Proximal | 0-Ip | 15 | No | Oxyntic | Surgery |
| 46 | F | Rd | Proximal | 0-IIb | 15 | No | Oxyntic | Med |
| 46 | M | No | Proximal | 0-IIb | 30 | No | Cardiac | Med |
| 46 | M | No | Middle | 0-IIc | 15 | Ulcer | Oxyntic | EMR |
| 47 | F | No | Proximal | 0-Ia | 30 | No | Oxyntic | Ablation |
| 48 | F | RD | Low | 0-IIb | 30 | No | Oxyntic | Surgery |
| 48 | F | RD | Low | 0-IIc | 30 | Bleeding | Oxyntic | Surgery |
| 51 | M | No | Proximal | 0-I | 30 | No | Mixed | Med |
| 51 | F | Diverticula | Low | 0-IIa + IIc | 20 | No | Mixed | EMR |
| 51 | M | No | Low | 0-Ia | 40 | No | Oxyntic | Med |
| 51 | M | No | Low | 0-Ib | 1 | No | Antral | Surgery |
| 52 | F | No | Low | O-IIa + III | 12 | Anal pain | Oxyntic | EMR |
| 53 | F | No | Low | 0-IIa | 35 | No | Oxyntic | Surgery |
| 58 | F | No | Low | 0-Ila | Oxyntic | Med | ||
| 63 | F | No | Low | 0-IIb | 30 | No | Oxyntic | ESD |
Discussion
Regarding the pathogenesis of HGM, Morrison[5] proposed a link to the incorrect differentiation of endodermal pluripotent stem cells during embryonic development. Wolff [6] expanded on this, categorizing HGM into two types: congenital developmental abnormalities if more than one type of epithelium is involved or if the entire ectopic mucosa layer consists of gastric fundic mucosa; acquired if the tissue is exclusively pyloric gland epithelium or dispersed principal and mural cells. The lesions in the present case align with congenital developmental abnormalities.
HGM is frequently associated with gastrointestinal abnormalities like duplication and diverticula, often appearing at the edge or inside diverticula, some displaying morphology resembling the diverticula. The simultaneous occurrence of gastrointestinal malformations and HGM may lead to frequent inflammatory stimulation, increasing the risk of bleeding, perforation, and heterogeneous hyperplasia.
A systematic review of rectal HGM cases and a clinicopathological classification could aid in determining clinical relevance and prognosis. Polypoid bulges (type I) are more prevalent among minors, possibly due to fewer endoscopies in children, while flat types (type II) are more common in adults, often incidentally found during colonoscopy in asymptomatic patients. Diagnosing HGM relies on pathology as it cannot be confirmed visually, emphasizing the importance of timely colonoscopy and biopsy or lesion removal for examination.
99 mTc scans can reveal the uptake point of ectopic gastric mucosa, particularly beneficial for lesions in challenging locations not covered by conventional gastroscopy and colonoscopy. However, the use of 99 mTc scans for all patients remains controversial [1,7,8].
Rectal HGM, though rare, should be considered in the differential diagnosis of rectal lesions or associated symptoms due to its acid secretion and potential co-infection with Helicobacter pylori (HP). Acid suppression therapy has proven effective in managing symptoms associated with acid secretion by HGM. HP eradication treatment is feasible for symptomatic rectal HGM co-infected with HP [9-11].
Studies have shown the carcinogenic potential of HGM, especially in cases with intraepithelial neoplasia. Long-standing rectal HGM may pose a risk of cancer, warranting endoscopic monitoring or resection if available [12].
Differentiating treatment approaches, conventional EMR and ESD, reveal the advantages of ESD in terms of better pathological evaluation, reduced residual lesions, and recurrence rates. ESD, despite being more challenging and risky than EMR, offers unique advantages for rectal HGM, particularly when lesions exceed 20 mm. ESD’s successful resection of the lesion in the present case demonstrates its effectiveness and potential as a preferred treatment modality for rectal HGM [13,14].
As more cases and studies emerge, further assessment of the predicted risk of HGM malignancy and treatment modalities will contribute to refining clinical management. In comparison to EMR, ESD’s superior pathological evaluation and positive prognosis in the following cases advocate for its promotion in the clinical management of rectal HGM [1].
In this case, the flat lesion in the rectum extended to the dentate line, classified as 0-IIa according to the Paris Classification and measuring approximately 35 mm. The EMR treatment trap tended to slide over the lesion and could not be secured. Although ESD could effectively overcome these limitations and achieve complete removal, the lesion’s proximity to the dentate line made a safe ESD approach unfeasible, leading us to perform a transanal excision instead.
Conclusion
Rectal HGM represents a rare but significant clinical entity. Treatment modalities, especially the shift towards ESD, demonstrate improved pathological evaluation and positive prognoses in following cases. The potential carcinogenicity of HGM underscores the importance of long-term endoscopic monitoring or resection when feasible. This review encourages ongoing research to refine clinical management strategies. As additional cases and studies emerge, further insights into the risk of malignancy and optimal treatment approaches will contribute to enhancing the overall care and outcomes for patients.
Declarations
Acknowledgments: The authors declare that there are no acknowledgments to be made for this work.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
References
- SIacopini, F, Gotoda, T, Elisei W, Rigato P, Montagnese F, Saito Y, et al. Heterotopic gastric mucosa in the anus and rectum: first case report of endoscopic submucosal dissection and systematic review. Gastroenterology Report. 2016; 4(3): 196-205
- Peng D, Qiu T, Chen S, Hu W, Fang T. A case report of heterotopic gastric mucosa in the rectum treated by endoscopic submucosal dissection and a systematic review. Medicine. 2023; 102(30): e3449.
- Ewell GH, Jackson RH. Aberrant gastric mucosa in the rectum with ulceration and hemorrhage. Wis Med J. 1939; 38: 641–3.
- Participants in the Paris Workshop. The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: novem- ber 30 to december 1. Gastrointest Endosc. 2003; 58(6 Suppl): S3–43
- Robbins SL. Third editionJ. Edgar Morison (Ed.) Foetal and Neonatal Pathology, Appleton-Century-Crofts (Educational Division, Meredith Corporation), New York (1970), 152 illustrations. 1971; 641 pages.
- Wolff M. Heterotopic gastric epithelium in the rectum: a report of three new cases with a review of 87 cases of gastric heterotopia in the alimentary canal. American journal of clinical pathology. 1971; 55(5): 604-616.
- Murray FE, Lombard M, Dervan P, et al. Bleeding from multifocal het- erotopic gastric mucosa in the colon controlled by an H2 antagonist. Gut. 1988; 29: 848–51.
- Rousseff T, Matthyssens L, Van Renterghem K, et al. Rectal red blood loss in a healthy toddler is not always a juvenile polyp. Acta Gastroenterol Belg. 2017; 80: 67–70.
- Galan AR, Katzka DA, Castell DO. Acid secretion from an esophageal inlet patch demonstrated by ambulatory Ph monitoring. Gastroenterology. 1998; 115: 1574–6.
- Alagozlu H, Simsek Z, Unal S, et al. Is there an association between helicobacter pylori in the inlet patch and globus sensation? World J Gastroenterol. 2010; 16: 42–7.
- Dye KR, Marshall BJ, Frierson HF Jr, et al. Campylobacter pylori colonizing heterotopic gastric tissue in the rectum. Am J Clin Pathol. 1990; 93: 144–7.
- Iwata H, Arai C, Koike Y, et al. Heterotopic gastric mucosa of the small intestine in laboratory beagle dogs. Toxicol Pathol. 1990; 18: 373–9.
- Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colo- rectal endoscopic submucosal dissection/endoscopic muco- salresection.DigEndosc. 2015; 27: 417–34.
- Iacopini F, Bella A, Costamagna G, et al. Stepwise training in rectal and colonic endoscopic submucosal dissection with differentiated learning curves. Gastrointest Endosc 2012; 76: 1188–96.
- Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler A, Orgill DP, For the SCARE Group. The SCARE 2018 Statement: Updating Consensus Surgical CAse REport (SCARE) Guidelines, International Journal of Surgery. 2018; 60: 132-136.