
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 6
Usefulness of the preceding EUS approach in the treatment strategy of acute cholangitis
Takumi Kinomoto; Kohsaku Ohnishi; Naoko Hayata; Akino Okamoto; Kazuki Aochi; Munehiro Ashida; Takahiro Tanimoto; Hiroki Murai; Tomohide Kurahashi; Motohiro Hirao; Takuya Yamada; Atsushi Hosui*; Naoki Hiramatsu
Department of Gastroenterology and Hepatology, Osaka Rosai Hospital, 1179-3 Nagasonecho, Kita Ward, Sakai, Osaka, Japan.
*Corresponding Author : Atsushi Hosui
Department of Gastroenterology and Hepatology,
Osaka Rosai Hospital, 1179-3 Nagasonecho, Kita
Ward, Sakai, Osaka, Japan.
Tel: 81-072-252-3561, Fax: 81-072-255-3349;
Email: hosui@osakah.johas.go.jp
Received : Feb 02, 2025
Accepted : Feb 25, 2025
Published : Mar 04, 2025
Archived : www.jcimcr.org
Copyright : © Hosui A (2025).
Abstract
Background/aims: The role of endoscopic ultrasonography (EUS) in managing acute cholangitis has not been established. The aim of this study was to evaluate the usefulness of EUS for acute cholangitis where common bile duct (CBD) stones could not be detected via other imaging methods.
Methods: Between April 2019 and March 2022, 145 patients were retrospectively analyzed. Regardless of the severity of acute cholangitis, EUS was performed for all patients whose CBD stones were not detected by CT scan. Endoscopic retrograde cholangiopancreatography (ERCP) was performed only if EUS detected CBD stones.
Results: There were 79 (mild), 54 (moderate), and 12 (severe) cases of cholangitis, respectively. CBD stones were detected in 92 patients. Conservative therapy was provided for the other 52 patients whose stones were not identified by EUS. Among these 52 patients, 3 were resistant to conservative therapy and 1 patient developed recurrent acute cholangitis. With this approach, 48 patients (33.1%) were successfully treated without ERCP. In cases of moderate cholangitis, 95.5% of patients were successfully treated without ERCP, which was not significantly different from the rate of mild severity.
Conclusions: Almost all acute cholangitis patients improved without emergent ERCP when EUS identified no CBD stones. EUS is valuable for determining the necessity of ERCP.
Keywords: Cholangiopancreatography; Cholangitis; Endosonography; Gallstones.
Citation: Hosui A, Kinomoto T, Ohnishi K, Hayata N, Okamoto A, et al. Usefulness of the preceding EUS approach in the treatment strategy of acute cholangitis. J Clin Images Med Case Rep. 2025; 6(3): 3493.
Introduction
Acute cholangitis is a disease characterized by bacterial infection of the common bile duct (CBD). In many instances, it manifests as a consequence of biliary obstruction, with CBD stones identified as the predominant etiological factor [1]. The Tokyo Guidelines 2018 (TG18) advocate endoscopic retrograde cholangiopancreatography (ERCP) as the foremost approach for biliary drainage in the treatment of acute cholangitis [2]. However, ERCP should be avoided if possible because it can cause severe complications, including pancreatitis [3,4].
Endoscopic ultrasonography (EUS) is known for its ability to identify CBD stones. A review of 2,673 cases from 27 references demonstrated a sensitivity and specificity of 95% each [5], indicating that sensitivity was superior to that of abdominal CT [6] (77%) and abdominal US [7] (45%). The sensitivity of magnetic resonance cholangiopancreatography (MRCP) was also reported to be between 80% and 100%, which is similar to that of EUS [8]. However, it is less effective in diagnosing small stones less than 5 mm in diameter [9]. In addition, EUS can be performed more safely than can ERCP [5] at the discretion of a gastroen terologist. When CBD stones are detected, the patient can be transferred to ERCP in the same session soon after EUS [10].
Previous studies have shown that EUS can prevent unnecessary ERCP in patients with suspected choledocholithiasis or acute pancreatitis [11-13]. However, there are no reports demonstrating the utility of EUS as a preliminary approach for acute cholangitis. In this study, we explored the usefulness of EUS before ERCP, for acute cholangitis where CBD stones were suspected from the clinical course and no stones could be detected on CT
Materials and methods
Patients and study design
We retrospectively reviewed the cases of 145 patients who were diagnosed with suspected or confirmed acute cholangitis at our hospital between April 2019 and March 2022 and whose CBD stones were never detected by imaging methods. Any patient with surgically altered anatomy and patient who suspected or already diagnosed with pancreatobiliary cancer were excluded from our study.
EUS/ERCP procedures
Endoscopic procedures were carried out by a senior endoscopist and young graduate trainee, a team with an experience of approximately 400 EUS and 700 ERCP procedures per annum. Midazolam was administered as a sedation method in all endoscopic procedure, with the procedure performed in the prone position. A linear scanning echoendoscope (GF-UCT260, Olympus Medical Systems, Tokyo, Japan) was used by our endoscopists for EUS examination. Positive identification of CBD stones was defined as a hyperechoic focus, with or without an acoustic shadow, which was observed within the stones. ERCP was performed using a duodenal videoscope (TJF-Q290V/JF260V, Olympus Medical Systems, Tokyo, Japan) for patients with poorly observed CBD or those with CBD stones. The method of drainage following bile duct cannulation and the decision to perform stone removal were left to the discretion of the endoscopist. When a detailed EUS examination revealed that CBD stones were not detected, a conservative approach involving antimicrobial agents was employed regardless of the severity of the cholangitis (Figure 1). Even among patients subjected to conservative management, ERCP-based biliary drainage was performed if there was no improvement in symptoms such as fever and abdominal pain, or in laboratory tests showing jaundice and inflammation within one to two days.
Definitions and assessment of outcomes
The diagnosis and severity of acute cholangitis were determined based on TG18. We defined patients who experienced “no recurrence with conservative treatment” as patients who were discharged from the hospital without drainage procedures such as ERCP during their stay and who experienced no recurrence of acute cholangitis or biliary cholelithiasis for a 3-month period after hospital discharge. The continuous variables presented as mean ± SD were analyzed by the Mann-Whitney U test. The category disguise was analyzed with Fisher’s exact test.
Results
Patient characteristics
EUS was performed in all 145 acute cholangitis patients with undetectable CBD stones, regardless of the severity of the cholangitis. The clinical characteristics of this cohort are shown in Table 1. There were 91 men and 54 women; the mean age was 75 ± 12 years. ERCP and endoscopic sphincterotomy (EST) had been performed for 10 patients. 79 patients were categorized as having mild (grade I) acute cholangitis, 54 as having moderate (grade II), and 12 as having severe (grade III) acute cholangitis. Based on the American Society for Gastrointestinal Endoscopy (ASGE) consensus guidelines for choledocholithiasis [14], 101 patients were classified as high (>50%), 44 were intermediate (10% to 50%) probability for choledocholithiasis: there were no patients of low (<10%) probability for choledocholithiasis. Plain CT was performed for all 145 patients, 111 of whom had contrast-enhanced CT. US was performed in 65 patients.
Detection of CBD stones via EUS
EUS was performed within 24 hours of the visit in 119 patients, and in 26 patients, it was performed within 24 to 48 hours of the visit. In 1 patient, EUS examination was not completed because the distal CBD could not be observed due to peripapillary diverticulum. All cases with the history of endoscopic sphincterotomy or cholecystectomy were adequately completed EUS examination. The median duration of the EUS procedure was 14 minutes (range 5-53). The mean diameter of the CBD was 7.3 ± 2.4 mm. Among the 144 patients for whom EUS examination was completed, CBD stones were detected in 92 patients (63%), and in 52 patients (36%), they were not detected (Table 2). The mean diameter of the CBD stones detected by EUS was 5.0 ± 2.7 mm. Specifically, small stones or debris measuring less than 5 mm were observed in 67 cases, stones ranging from 5 to 10 mm in 20 cases, and 5 cases of stones exceeding 10 mm, which were difficult to detect by CT. According to the severity of acute cholangitis, EUS revealed the presence of stones in 50 patients (64%) with mild acute cholangitis, 32 (59%) with moderate cholangitis, and 10 (83%) with severe cholangitis. The cases of high probability and intermediate probability of choledocholithiasis based on ASGE consensus guidelines showed no significant differences in the detection of CBD stones. There were no complications caused by EUS examination.
Outcomes and follow-up
In 92 patients with CBD stones detected by EUS and 1 patient with insufficient EUS examination, all patients underwent ERCP. In all cases of 93 patients, successful bile duct cannulation was achieved, and CBD stones were identified by cholangiography in all cases. Among these, EST was performed in 37 cases. Biliary drainage was carried out in 80 cases, and stone removal was performed in 13 cases. The median procedure time for ERCP was 22 minutes (range: 8-178 minutes), with technical success was achieved in all cases. Complications associated with ERCP included pancreatitis in 6 cases (all cases were mild pancreatitis) and bleeding following EST in 5 cases. In 52 patients without CBD stones according to EUS, ERCP was not performed, and these patients were treated conservatively. Three patients experienced limited improvement in cholangitis, so ERCP was conducted on the following day for 2 patients and 4 days after the EUS procedure for 1 patient. The other 49 patients received conservative treatment and were discharged without undergoing ERCP during their hospital stay. One patient experienced a recurrence of acute cholangitis 2-months after discharge. Of these 4 patients who underwent conservative treatment based on EUS results but needed additional bile duct drainage by ERCP, 3 had mild acute cholangitis, and 1 had moderate acute cholangitis. All of these 4 patients followed by clinical improvement after additional ERCP. As a result, using this treatment strategy, ERCP could be avoided in 33.1% (48/145) of patients. Among the 52 patients identified as having no CBD stones by EUS, 92.3% (48/52) had no recurrence, indicating that these patients recovered from acute cholangitis without an ERCP procedure. Based on the severity of acute cholangitis, the no-recurrence rate of EUS-negative patients was 89.3% (25/28) for mild cholangitis and 95.5% (21/22) for moderate cholangitis. There was no significant difference in treatment outcomes between these two groups (p>0.999) (Table 3).
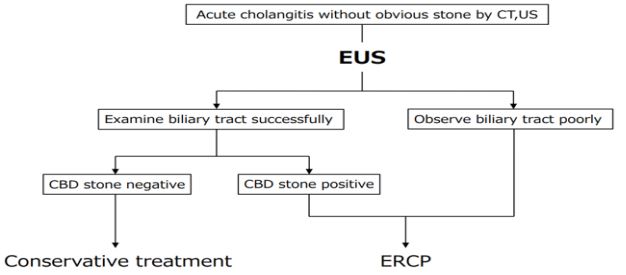
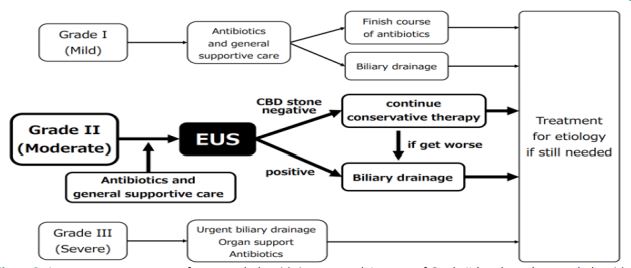
Table 1: Baseline characteristics of Patients
| Overall (n=145) | ||
|---|---|---|
| Age (y) | 75±12 | |
| Sex (M/F) | 91/54 | |
| Previous ERCP | 10 (7%) | |
| Previous cholecystectomy | 16 (11%) | |
| Gallbladder stones | 100 (69%) | |
| Symptoms | ||
| Fever (>38OC) | 50 (35%) | |
| Abdominal pain | 94 (65%) | |
| Laboratory fiding(mean±SD) | ||
| AST (IU/L) | 301±518 | |
| ALT (IU/L) | 240±272 | |
| Total bilirubin (mg/dL) | 2.9±3.1 | |
| ALP (IU/L) | 375±326 | |
| GGT (IU/L) | 380±361 | |
| Albumin (g/dL) | 3.5±0.6 | |
| WBC (/mm3) | 10,228±4,822 | |
| Diagnosis of acute cholangitis | ||
| Suspected diagnosis | 77 (53%) | |
| Definite diagnosis | 68 (47%) | |
| Severity ofcholangitis | ||
| Grade I | 79 (54%) | |
| Grede II | 54 (37%) | |
| Grade III | 12 (8%) | |
| ASGE guidelines choledocholithiasis | ||
| High probability (>50%) | 101 (70%) | |
| Intermediate probability (10%–50%) | 44 (30%) | |
| Low probability (<10%) | 0 | |
| Imaging testsperformed prior to EUS | ||
| CT scan | 145 (100%) | |
| contrast enhanced CT | 111 (77%) | |
| abdominal US | 65 (45%) | |
| MRCP | 3 (2.1%) | |
| ERCP:Endoscopic Retrograde Cholangiopancreatography; AST: Aspartate Aminotransferase; ALT:Alanine Aminotransferase; ALP: Alkaline Phosphatase; GGT: g-GlutamylTransferase; ASGE: American Society for Gastrointestinal Endoscopy; EUS:Endoscopic Ultrasonography; MRCP: Magnetic Resonance Cholangiopancreatography. | ||
Table 2: CBD stones detected on EUS.
| Positive | Negative | Unclear | P-valuea) | ||
|---|---|---|---|---|---|
| Total | 92(63%) | 52(36%) | 1 (1%) | ||
| Severity ofcholangitis | 0.314 | ||||
| Grade I | 50(64%) | 28(35%) | 1 (1%) | ||
| Grade II | 32(59%) | 22(41%) | 0 | ||
| Grade III | 10(83%) | 02(17%) | 0 | ||
| ASGE guidelines | 0.162 | ||||
| High probability | 67(66%) | 33(33%) | 1 (1%) | ||
| Intermediate probability | 25(57%) | 19(43%) | 0 | ||
| a)Fisher's exact test | |||||
Table 3: No-recurrence rate of acute cholangitis in EUS negative group.
| No stones detected by EUS | No recurrence | P-valuea) | |
|---|---|---|---|
| Total | 52 | 48(92.3%) | >0.999 |
| GradeI | 28 | 25(89.3%) | |
| GradeII | 22 | 21(95.5%) | |
| GradeIII | 2 | 2 (100%) | |
| a)Fisher's exact test | |||
Discussion
This study is the first to demonstrate the usefulness of EUS in the treatment of acute cholangitis when the cause of cholangitis cannot be identified by CT. The TG18 is commonly used as a guideline for the diagnosis and treatment of acute cholangitis and includes recommendations for the appropriate time to drain the biliary tract based on the severity of the disease [2].
The treatment criteria were as follows:
① Mild acute cholangitis, in which biliary drainage is recommended only when a patient does not respond to initial treatment, including antibiotics;
② Moderate acute cholangitis, in which biliary drainage is recommended for the first time; and
③ Severe acute cholangitis, in which emergent biliary drainage is needed after the patient’s general condition improved with initial treatment and respiratory/circulatory management. Despite the severity of cholangitis, patients sometimes improve without biliary drainage if small stones or debris spontaneously pass from the CBD to the duodenum [15]. It is difficult to distinguish only by CT whether these stones and debris remain in the CBD or pass through the CBD to the duodenum.
In our study, EUS was conducted for all patients with acute cholangitis whose CBD stones were undetectable on imaging, regardless of the severity of cholangitis. As a result, EUS made it possible to avoid unnecessary ERCP in one-third of all patients, and 92% of those patients with undetectable CBD stones on EUS experienced no recurrence without biliary drainage on ERCP. Notably, there were no significant differences between the norecurrence rates for mild and moderate cholangitis patients. These findings suggest the usefulness of EUS as a treatment strategy for the moderate acute cholangitis (Figure 2). Early bili ary drainage is not required for the moderate acute cholangitis patients with no stones. They can be treated similarly to patients with mild cholangitis: conservative treatment, including antibiotics, should be given first, and ERCP should be performed only if they exhibit resistance to the treatment. This treatment approach is beneficial for preventing ERCP with safety.
Although this study shows certain usefulness of EUS for moderate acute cholangitis, the suitability of this strategy for mild and severe cholangitis needs additional examinations. In patients with mild cholangitis or those with no symptoms, biliary obstruction is suspected to be less severe or stones have passed. In these cases, it may be preferable to treat conservatively as recommended by the TG18, and subsequently performed diagnostic evaluations such as EUS or MRCP to assess the presence of CBD stones. On the other hand, in cases of severe cholangitis, this study indicated the presence of CBD stones in almost all cases. Severe cholangitis represents a high risk of fatality, and there is a risk of missing the timing for drainage in the event of deterioration. Additionally, performing EUS may delay the conduct of ERCP. Therefore, it may be preferable to adopt a strategy of performing ERCP without preceding EUS, as currently recommended by TG18.
In our study, we performed CT scan for the diagnosis of acute cholangitis, and subsequently conducted EUS for the detection of CBD stones: the use of MRCP prior to EUS was infrequent. MRCP has been reported to demonstrate comparable sensitivity and specificity to EUS in the detection of CBD stones [8], however, it is also reported that MRCP is less effective in diagnosing small stones less than 5 mm in diameter [9], which were frequently observed in our cohort. Additionally, as noted in TG18, some facilities may find it difficult to provide rapid MRCP assessments because of limited accessibility. This can lead to a risk of delays in diagnosis and treatment for urgent cases of acute cholangitis. Although there is no doubt regarding the importance of MRCP in diagnosing choledocholithiasis, EUS may have advantages in the management of acute cholangitis because it needs for urgent diagnosis and treatment.
Notably, in 4 patients in this study, EUS detected no CBD stones, but additional ERCP was later needed. In 2 of these cases, there might be false-negative EUS outcomes or suspected gallstone fallout from the gallbladder post-EUS procedure. In 1 patient, EUS was performed on the day of hospitalization, and no CBD stones were detected. We diagnosed that bile duct wall thickening was caused secondary to acute cholangitis. Conservative treatment, including antibiotics, was initiated and led to an improvement in the inflammatory response. However, due to the lack of improvement in obstructive jaundice, ERCP was conducted for further evaluation and drainage on the third day of hospitalization. Cholangiography revealed a bile duct stricture and eosinophilic cholangitis was diagnosed by histological analysis based on biopsy of the bile duct. In another patient, ERCP was needed for diagnosis even though cholangitis was not the primary issue. We should focus on the possibility that EUS might miss stones because its accuracy depends on the endoscopists’ skills [16,17]. The thickened bile duct walls and dilated bile ducts from acute cholangitis can make it difficult to diagnose by EUS [11]. Even if stones are not detected via EUS, the clinical course should be closely monitored, and the appropriate duration of bile duct drainage should never be missed if the degree of cholangitis does not improve.
Due to the single-center retrospective study, there are several limitations in this study. Firstly, there is a potential for bias in the selection of cases for EUS, as well as in the outcomes of EUS, the details of ERCP procedures, treatment courses, and other related factors. Secondly, in our facility, we have good access to endoscopic examinations and endoscopists who can urgently perform EUS examinations, allowing for rapid assessment of the bile ducts and determination of the presence of CBD stones. However, considering the risk that prolonged EUS may delay drainage via ERCP, it remains unclear whether this strategy can be generalized to all facilities. Therefore, further studies in large-scale and compared with current guideline treatment strategies are needed.
Conclusion
In conclusion, preemptively conducting EUS in patients with acute cholangitis in which CBD stones are not identified by CT allowed us to choose patients who needed ERCP and prevent unnecessary procedures in approximately one-third of all patients. Specifically, moderate cholangitis can be effectively managed without ERCP if EUS determines the absence of CBD stones. Our study offers new insights to treatment strategy of acute cholangitis and that may improve patient outcomes.
Declarations
Conflict of interests: The authors have no potential conflicts of interest.
Funding: None
Acknowledgments: None
Author contributions: Conceptualization: TK, KO, TT, MH, AH, NH; Data curation: TK; Formal analysis: TK, KO, TK; Methodology: TK, KO, TT, MH, AH, NH; Project administration: TK, KO, AH; Resources: TY, AH, NH; Supervision: KO, AH, NH; Validation: TK, KO, AH; Visualization: TK; Writing-original draft: TK, KO, AH; Writing-review & editing: all authors.
Ethics statement: [Approval of the research protocol by an Institutional Reviewer Board]. This study was approved by the Institutional Review Board of Osaka Rosai Hospital and was conducted according to the principles of the Declaration of Helsinki. The Approval number is “2023-8”.
References
- Gomi H, Takada T, Hwang T-L, et al. Updated comprehensive epidemiology, microbiology, and outcomes among patients with acute cholangitis. J Hepato-Biliary-Pancreat Sci. 2017; 24: 310– 8
- Miura F, Okamoto K, Takada T, et al. Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis. J Hepato-Biliary-Pancreat. Sci 2018; 25: 31– 40.
- Chandrasekhara V, Khashab MA, Muthusamy VR, et al. Adverse events associated with ERCP. Gastrointest Endosc. 2017; 85: 32–47.
- Masci E, Toti G, Mariani A, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001; 96.
- Tse F, Liu L, Barkun AN, et al. EUS: a meta-analysis of test performance in suspected choledocholithiasis. Gastrointest Endosc. 2008; 67: 235–44.
- Tseng C-W, Chen C-C, Chen T-S, et al. Can computed tomography with coronal reconstruction improve the diagnosis of choledocholithiasis? J Gastroenterol Hepatol. 2008; 23: 1586–9.
- O’Connor HJ, Hamilton I, Ellis WR, et al. Ultrasound detection of choledocholithiasis: prospective comparison with ERCP in the postcholecystectomy patient. Gastrointest Radiol. 1986; 11: 161–4.
- Rhaiem R, Piardi T, Renard Y, et al. Preoperative magnetic resonance cholangiopancreatography before planned laparoscopic cholecystectomy: is it necessary? J Res Med Sci Off J Isfahan Univ Med Sci. 2019; 24: 107.
- Jendresen MB, Thorbøll JE, Adamsen S, et al. Preoperative routine magnetic resonance cholangiopancreatography before laparoscopic cholecystectomy: a prospective study. Eur J Surg Acta Chir. 2002; 168: 690–4.
- Vila JJ, Kutz M, Goñi S, et al. Endoscopic and anesthetic feasibility of EUS and ERCP combined in a single session versus two different sessions. World J Gastrointest Endos. 2011; 3: 57–61.
- Choi YH, Lee YS, Lee SH, et al. Role of EUS at high risk for choledocholithiasis without severe cholangitis and visible stone on cross-sectional imaging: A multicenter randomized clinical trial. Endosc Ultrasound. 2021; 10: 455–62.
- Jeon TJ, Cho JH, Kim YS, et al. Diagnostic Value of Endoscopic Ultrasonography in Symptomatic Patients with High and Intermediate Probabilities of Common Bile Duct Stones and a Negative Computed Tomography Scan. Gut Liver. 2017; 11: 290–7.
- Quispel R, van Driel LMWJ, Veldt BJ, et al. The utility and yield of endoscopic ultrasonography for suspected choledocholithiasis in common gastroenterology practice. Eur J Gastroenterol Hepatol. 2016; 28: 1473–6.
- Buxbaum JL, Abbas Fehmi SM, Sultan S, et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest Endosc. 2019; 89: 1075-1105. e15.
- V L, Rj M. Spontaneous passage of common bile duct stones in jaundiced patients. Hepatobiliary Pancreat Dis Int HBPD INT. 2011; 10.
- DE Angelis CG, Rizza S, Rizzi F, et al. Training in advanced biliopancreatic endoscopy. Minerva Gastroenterol. 2022; 68: 121– 32.
- Sachin W, Matthew H, Rajesh K, et al. Variation in Aptitude of Trainees in Endoscopic Ultrasonography, Based on Cumulative Sum Analysis. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2015; 13.