
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A rare vascular combination in an adult: Hypoplasia of the right pulmonary artery and veins
Abdelkader Sqalli Houssaini*; Ikram Sarsar; Yahya El Harras; Omar El Aoufir; Laila Jroundi; Ola Messaoud
Department of Emergency Radiology, Ibn Sina University Hospital, Mohammed V University, Rabat, Morocco.
*Corresponding Author : Houssaini AS
Department of Emergency Radiology, Ibn Sina
University Hospital, Mohammed V University,
Rabat, Morocco.
Email: sqalliabdelkader@gmail.com
Received : Jan 14, 2025
Accepted : Feb 26, 2025
Published : Mar 05, 2025
Archived : www.jcimcr.org
Copyright : © Houssaini AS (2025).
Abstract
Combined unilateral hypoplasia of the pulmonary artery and veins is an extremely rare congenital anomaly, mostly described in children and exceptionally seen in adults. It is usually manifested by ipsilateral lung hypoplasia, reduced lung vascularization, and compensatory contralateral vessel hyperplasia. Contrast-enhanced Computed Tomography (CT) typically reveals a reduction in pulmonary artery caliber, absent or hypoplastic pulmonary veins, and lung parenchymal changes such as interlobular septal thickening and ground-glass attenuation. Patients may present with recurrent respiratory infections or remain asymptomatic until adulthood. We report a case of an adult patient with combined hypoplasia of the right pulmonary artery and veins, diagnosed incidentally during an evaluation for chronic respiratory symptoms. Angio-CT confirmed the diagnosis. This case highlights the importance of recognizing such rare vascular anomalies to ensure accurate diagnosis and appropriate clinical management.
Keywords: Pulmonary artery hypoplasia; Pulmonary vein hypoplasia; CT angiography; Congenital malformation.
Citation: Houssaini AS, Sarsar I, Harras YE, Aoufir OE, Jroundi L, et al. A rare vascular combination in an adult: Hypoplasia of the right pulmonary artery and veins. J Clin Images Med Case Rep. 2025; 6(3): 3495.
Introduction
Unilateral hypoplasia of the pulmonary artery and veins is an extremely rare congenital anomaly caused by embryologic developmental failure [1]. This condition often leads to ipsilateral lung fibrosis [2,3]. While isolated hypoplasia of the pulmonary artery or veins has been more frequently reported, the combination of both anomalies is exceptionally uncommon, particularly in adults [4,5].
Clinically, patients may present with nonspecific symptoms that can mimic other pulmonary conditions such as tuberculosis or interstitial lung diseases [1]. Imaging, especially angio-CT, is essential for the diagnosis, showing both vascular and parenchymal abnormalities. A thorough analysis is necessary to eliminate differential diagnoses such as chronic thromboembolic pulmonary hypertension, Scimitar syndrome, and fibrosing mediastinitis [4].
This report highlights a case of combined hypoplasia of the right pulmonary artery and veins diagnosed incidentally during the evaluation of chronic respiratory symptoms. It aims to underline the clinical and imaging features crucial for identifying such rare anomalies and preventing diagnostic delays.
Case report
A 58-year-old female presented with chronic dry cough and progressive dyspnea over the past five years. The patient reported recurrent respiratory infections since early adulthood, treated with antibiotics. There was no history of hemoptysis, chest pain, or pulmonary embolism.
On physical examination, the patient was apyretic, and her oxygen saturation was normal. Laboratory tests, including a complete blood count and inflammatory markers, were within normal limits. Sputum analysis for tuberculosis was negative.
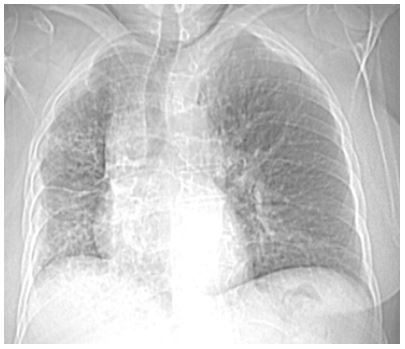
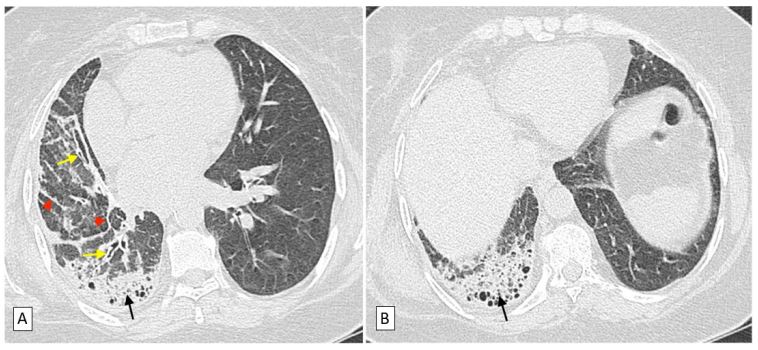
Initial chest CT showed reduced right lung size with interlobular reticulation (Figure 1). A follow-up non-contrast thoracic CT demonstrated signs of diffuse subpleural and basal fibrosis in the right lung, characterized by interlobular septal thickening, traction bronchiectasis, and subpleural honeycombing (Figure 2). The diagnosis of Usual Interstitial Pneumonia (UIP) was considered.
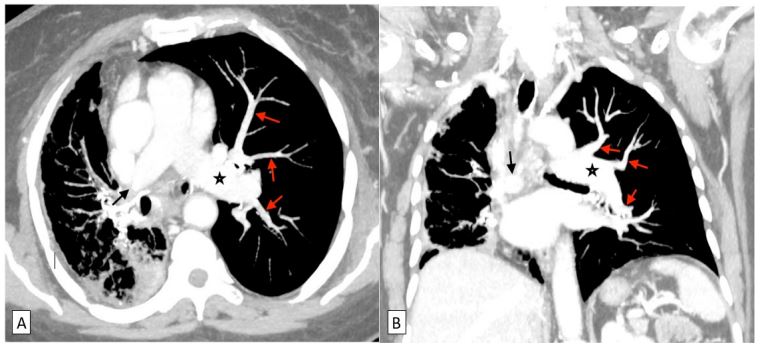
Due to persistent symptoms despite symptomatic treatment, a contrast-enhanced CT was performed. The angio-CT revealed the following:
• The main pulmonary artery and left pulmonary artery were normally opacified.
• The right pulmonary artery was only opacified at its origin, with an abrupt cutoff and complete absence of distal branches (Figure 3).
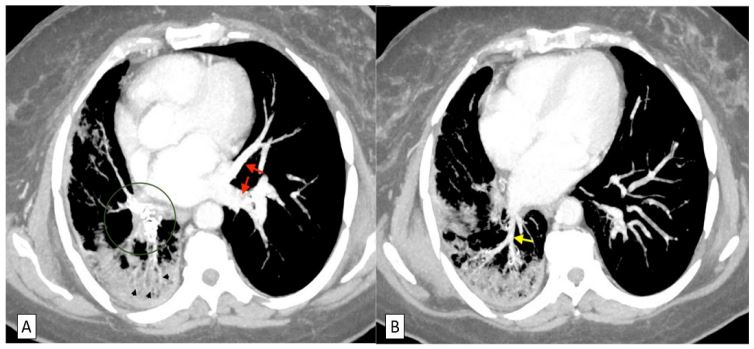
• Hypoplasia of the right pulmonary veins was observed. The right posterior pulmonary vein measured 3 mm near its insertion into the left atrium, while the right anterior vein was visualized only at its insertion, measuring 2 mm in diameter (Figure 4).
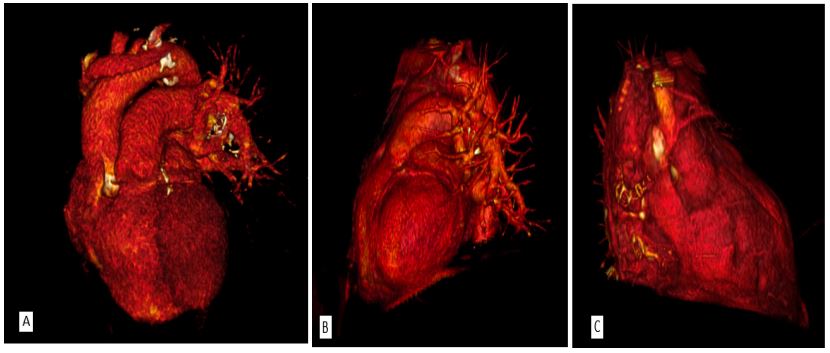
• Significant collateral circulation from hypertrophied bronchial arteries and systemic veins was noted. Diffuse tracheobronchial calcifications and small mediastinal lymph nodes were also identified. 3D reconstructions provided a comprehensive overview of the vascular anomalies (Figure 5).
• The findings suggested unilateral pulmonary fibrosis secondary to vascular hypoplasia. A multidisciplinary approach involving pulmonology and cardiology was adopted. Respiratory function tests revealed a restrictive ventilatory pattern. The patient’s significant collateral circulation explained the delayed onset of symptoms.
Discussion
The simultaneous hypoplasia of the right pulmonary artery and veins is an exceptionally rare condition, particularly in adults. It results from embryologic developmental failure. The right pulmonary artery originates from the sixth aortic arch during embryogenesis [2,5]. Improper separation of the truncus arteriosus can cause hypoplasia or interruption of the artery. Hypoplasia of the pulmonary veins is due to incomplete incorporation of the common pulmonary vein into the left atrium [8].
Radiological evaluation is essential for diagnosis. Chest radiographs often show asymmetry in lung volumes, with the affected side exhibiting volume loss and mediastinal shift. AngioCT is the gold standard for evaluating vascular anomalies [6].
Differential diagnoses include chronic thromboembolic pulmonary hypertension, scimitar syndrome, and fibrosing mediastinitis. Management depends on symptom severity. Conservative treatment is suitable for asymptomatic patients. Symptomatic cases may require bronchial artery embolization, pneumonectomy, or lung transplantation [4,8].
Conclusion
The rare combination of right pulmonary artery and vein hypoplasia highlights the importance of a multidisciplinary approach for accurate diagnosis and management [8]. Advances in imaging modalities, particularly CT angiography and threedimensional reconstructions, have significantly improved our understanding of this condition, enabling precise characterization and tailored treatment strategies [4]. Further studies are warranted to explore long-term outcomes and optimal management protocols for these patients [6].
Declarations
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest: The authors declare no conflict of interest in preparing this article.
Ethics approval: Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent: Written informed consent was obtained from the patient for their anonymized information to be published in this article.
References
- Carter J, Maldonado F, Villarraga HR, Ryu JH, Decker PA, Abrahams CP. Congenital abnormalities of the ulmonary arteries in adults: a practical approach. Chest. 2014; 146: 1078-1088.
- Dillman JR, Yarram SG, Hernandez RJ. Imaging of pulmonary venous developmental anomalies. Radiographics. 2012; 29: 1177- 1193.
- Frazier AA, Rosado-de-Christenson ML, Galvin JR. Unilateral pulmonary vein atresia: radiologic findings. Radiology. 2000; 217: 435-443.
- Heyneman LE, Nolan RL, Harrison JK, McAdams HP. Congenital unilateral pulmonary vein atresia: radiologic findings in three adult patients. AJR Am J Roentgenol. 2001; 177: 681-685.
- Ten Harkel AD, Blom NA, Ottenkamp J. Isolated unilateral absence of a pulmonary artery: a case report and review of the literature. Chest. 2002; 122: 1471-1477.
- Cung-Van Cong, Ly TT, Nguyen MD. Unilateral pulmonary vein atresia: literature overview and case report. Radiology Case Reports. 2022; 17: 1313-1317.
- Sakai T, Murayama S, Soeda H, et al. Imaging of diffuse pulmonary diseases: evaluation with high-resolution CT. Radiographics. 2002; 22: 989-1002.
- Joanna D, Chavhan GB, Temple M, Amaral JG, Moineddin R, Ho M. Congenital anomalies of the pulmonary arteries: an imaging overview. Br J Radiol. 2018; 91: 20180150.
- Turner A, Nicholson AA, Richardson DL, et al. Pulmonary atresia and major aortopulmonary collateral arteries. Radiographics. 2000; 20: 1441-1450.
- Rene P, Castaing Y, Bouchama A, et al. Pulmonary artery atresia with pulmonary hypertension. Chest. 1995; 107: 613-617.