
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Catastrophic fat emboli syndrome: When magnetic resonance imaging isn’t an option
Ankur Goswami*; Julie A Kromm
Department of Critical Care Medicine, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
*Corresponding Author : Ankur Goswami
Department of Critical Care Medicine, Cumming
School of Medicine, University of Calgary, Calgary,
AB, Canada.
Email: ankur.goswami@ucalgary.ca
Received : Jan 06, 2025
Accepted : Feb 27, 2025
Published : Mar 06, 2025
Archived : www.jcimcr.org
Copyright : © Goswami A (2025).
Abstract
Fat Emboli Syndrome (FES) represents an uncommon cause of coma in acute trauma patients. Given nonspecific clinical findings, diagnosis is frequently dependent on MRI. We present a case of FES leading to severe cerebral ischemia and refractory intracranial hypertension, where MRI could not be safely pursued.
Keywords: Fat Emboli Syndrome (FES); Severe cerebral ischemia; Refractory intracranial hypertension.
Citation: Goswami A, Kromm JA. Catastrophic fat emboli syndrome: When magnetic resonance imaging isn’t an option. J Clin Images Med Case Rep. 2025; 6(3): 3497.
Introduction
Fat Emboli Syndrome (FES) describes a constellation of clinical findings attributable to fat globule emboli from long bone and/or pelvic fractures. Disease pathogenesis is attributed to microcirculatory dysfunction in a variety of organs, resulting in a classic triad of hypoxemia, neurologic dysfunction, and petechial rash [1]. Despite a significant number of patients with long bone compromise showing evidence of circulating fat emboli, only a minority of patients develop FES (approximately 1 in 111 to 1 in 385) [1,2].
Several diagnostic criteria have been proposed, however Gurd’s is most commonly used [3]. CT and MRI are useful for characterizing the degree of central nervous system involvement; however findings are non-specific. While MRI is preferred given its high sensitivity and ability to detect characteristic findings of cytotoxicity from fat emboli early in the disease course4 patients may be too unwell to undergo such imaging and CT may be the only available option.
Mortality for this condition is reported to be anywhere from 7 to 36% [1]. Approximately 80% of patients require intensive care unit admission, and 60% undergo mechanical ventilation [5]. Case reports indicate recovery from severe FES is possible, although prolonged disorders of consciousness are reported [6- 8].
Case report
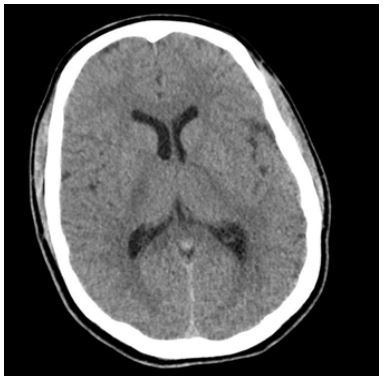
A healthy, 18-year-old male sustained a dirt bike accident resulting in multiple long bone fractures including a comminuted right femur, left tibia, left fibula, and right humeral head fractures. Upon presentation, his Glasgow Coma Scale (GCS) was 15 with no reported headache or neurological deficits except amnesia. His initial CT head was normal (Figure 1).
Shortly after his fractures had been reduced, he decompensated with fever (39.4OC), tachypnea, hypoxemia, tachycardia, acute anemia, thrombocytopenia, and a drop in GCS to 7. He was intubated and admitted to the intensive care unit. Repeat CT head 16 hours from previous demonstrated diffuse cerebral edema and basal cistern effacement, while CT angiography of his head and neck showed no abnormalities. Given the clinical context he was diagnosed with Fat Emboli Syndrome (FES). He had no documented hypotension to have caused watershed in farctions, nor biochemical evidence of disseminated intravascular coagulation, no cardiac trauma or shunt to have caused diffuse cerebral thromboembolisms, nor was his presenting imaging and exam consistent with diffuse axonal injury. His gas exchange following intubation was stable on an inspired fraction of oxygen of 25-30% and Positive End Expiratory Pressure (PEEP) of 8 to 10 cm H20.
An external ventricular drain was placed to monitor Intracranial Pressure (ICP) and cerebral autoregulation. Escalating therapies including hyperosmolar agents, sedatives, barbiturates, neuromuscular blockade, and hypothermia were used to manage intracranial hypertension. He was also initiated on pulse dose glucocorticoids for 72 hours – emerging evidence suggests its use in preventing FES and improving hypoxia [9].
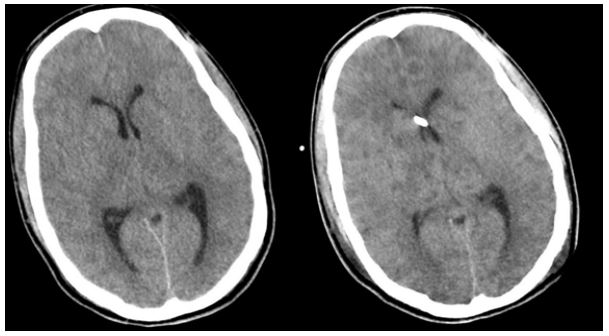
Given his extremely high ICP (30-60 mmHg), it was deemed unsafe to pursue Magnetic Resonance Imaging (MRI). Repeat CT demonstrated worsening edema and multifocal areas of reduced attenuation involving both grey and white matter similar to a starfield pattern (Figure 2). The patient subsequently underwent a bifrontal hemicraniectomy for refractory intracranial hypertension (Figure 3), with ongoing evolution of ischemia and hemorrhagic conversion.
Despite these interventions, he continued to decline with refractory intracranial hypertension, a GCS of 3 and fixed pupils. In discussion with consulting services, his injury was ultimately felt to not be survivable, and after meeting with his family life sustaining therapy was withdrawn.

Discussion/conclusion
Coma in critically ill trauma patients can have a broad differential. Neuroimaging such as MRI is commonly pursued for diagnostic clarity, prognostication and to guide decision making.
We present a case where management was pursued without MRI given patient safety considerations. Though it is a frequently utilized imaging modality in the setting of a comatose polytrauma patient, our case provides guidance on a scenario where a patient may be managed without. It has implications for patients to sick to tolerate transfer out of the intensive care unit and limited resource settings.
References
- Luff D, Hewson DW. Fat embolism syndrome. BJA Educ. 2021; 21: 322-8.
- Stein PD, Yaekoub AY, Matta F, Kleerekoper M. Fat embolism syndrome. Am J Med Sci. 2008; 336: 472-7.
- Gurd AR. Fat embolism: an aid to diagnosis. J Bone Joint Surg Br. 1970; 52: 732-7.
- Parizel PM, Demey HE, Veeckmans G, et al. Early diagnosis of cerebral fat embolism syndrome by diffusion-weighted MRI (starfield pattern). Stroke. 2001; 32: 2942-4.
- Tsai SHL, Chen CH, Tischler EH, et al. Fat Embolism Syndrome and in-Hospital Mortality Rates According to Patient Age: A Large Nationwide Retrospective Study. Clin Epidemiol. 2022; 14: 985-96.
- Hermann B, Brisson H, Langeron O, et al. Unexpected good outcome in severe cerebral fat embolism syndrome. Ann Clin Transl Neurol. 2018; 5: 988-95.
- Manousakis G, Han DY, Backonja M. Cognitive outcome of cerebral fat embolism. J Stroke Cerebrovasc Dis. 2012; 21: 906 e1-3.
- Wang W, Chen W, Zhang Y, Su Y, Wang Y. Post-traumatic cerebral fat embolism syndrome with a favourable outcome: a case report. BMC Neurol. 2021; 21: 82.
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009; 52: 386-93.