
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Docetaxel-induced interstitial pneumonitis in metastatic breast carcinoma: A case report
Bana Mary Manishaa1*; Bhargav Shreeram Gundapuneedi2
1Department of Pulmonology and Critical Care, Shri Sathya Sai Medical College and Research Institute, India.
2Department of Radiation Oncology, Jawaharlal Institute of Postgraduate Medical Education and Research, India.
*Corresponding Author : Bana Mary Manishaa
Department of Pulmonology and Critical Care, Shri
Sathya Sai Medical College and Research Institute,
Chennai, India.
Email: banamary.manishaa@student.sbvu.ac.in
Received : Jan 20, 2025
Accepted : Feb 27, 2025
Published : Mar 06, 2025
Archived : www.jcimcr.org
Copyright : © Manishaa BM (2025).
Abstract
Introduction: Chemotherapy-induced pulmonary toxicity is a rare but potentially life-threatening complication, encompassing a broad spectrum of manifestations, including interstitial pneumonitis. Docetaxel, a taxane-based chemotherapy agent widely used in the treatment of various malignancies, is known to cause interstitial pneumonitis, particularly in patients with breast carcinoma.
Case summary: We report a case of a 44-year-old premenopausal woman with metastatic breast carcinoma (cT4b N2a M1) who developed docetaxel-induced interstitial pneumonitis. The patient had a history of hypothyroidism and presented with a lump in the right breast. Imaging studies revealed a suspicious mass with associated nodal metastasis, and a biopsy confirmed invasive ductal carcinoma. Following palliative chemotherapy with Paclitaxel and Carboplatin, the patient underwent palliative mastectomy and adjuvant chemotherapy with Capecitabine. The disease later progressed to brain metastases, for which the patient received whole-brain radiotherapy and was started on Docetaxel. After the first cycle of Docetaxel, the patient developed acute respiratory symptoms. Despite an extensive workup to rule out other causes and treatment with high-dose corticosteroids, the patient succumbed to type-2 respiratory failure.
Discussion: Docetaxel-induced interstitial pneumonitis, although rare, has a high mortality rate and presents diagnostic challenges. The diagnosis is primarily based on clinical and radiological findings, supported by the exclusion of other differential diagnoses such as opportunistic infections and pulmonary embolism. The pathogenesis of this condition involves immune-mediated hypersensitivity reactions, and the incidence is related to the chemotherapy schedule. Early recognition and prompt initiation of high-dose corticosteroid therapy are critical for improving patient outcomes.
Conclusion: This case underscores the importance of vigilant monitoring, early identification, and multidisciplinary management in patients receiving taxane-based chemotherapy to mitigate the risks of interstitial pneumonitis and improve survival outcomes. Ongoing research is needed to understand the mechanisms of taxane-induced pulmonary toxicity better and to develop strategies for its prevention and management.
Keywords: Multidisciplinary approach; Docetaxel; Chemotherapy; Metastatic carcinoma of the breast; Drug-induced interstitial pneumonitis.
Citation: Manishaa BM, Gundapuneedi BS. Docetaxel-induced interstitial pneumonitis in metastatic breast carcinoma: A case report. J Clin Images Med Case Rep. 2025; 6(3): 3498.
Introduction
Chemotherapy-induced pulmonary toxicity encompasses a broad range of manifestations, including interstitial pneumonitis, organizing pneumonia, diffuse alveolar damage, alveolar haemorrhage, and noncardiogenic pulmonary oedema. Agents reported to cause Acute Interstitial Pneumonia (AIP) in cancer patients include docetaxel, paclitaxel, methotrexate, pemetrexed, bortezomib, fludarabine, gemcitabine, ifosfamide, irinotecan, oxaliplatin, thalidomide, lenalidomide, and vinca alkaloids [1]. AIP is marked by rapidly progressing dyspnea developing over days to weeks, leading to respiratory failure in patients who do not have preexisting lung disease or extrathoracic conditions known to affect the lungs [2]. The incidence of drug-induced pneumonitis in breast cancer is 1.7% [3]. Taxanes like Docetaxel and Paclitaxel are highly effective chemotherapy agents utilized in the treatment of various malignancies, especially in breast cancer management [4]. Drug-induced pneumonitis is a rare complication (1-5%) with taxane-based chemotherapy [5]. Pulmonary toxicities associated with taxane use have been documented in numerous reports, particularly in patients with non-small cell lung cancer, breast cancer, and prostate cancer [6-8]. We report a case of metastatic carcinoma of the breast, who developed interstitial pneumonitis as a complication of Docetaxel.
Case report
A 44-year-old premenopausal woman with a history of hypothyroidism on regular medication presented with a lump in her right breast for 2 months with no history of trauma, pain, fever, nipple discharge or skin ulceration. Mammogram revealed a large lobulated hypoechoic lesion with internal vascularity in the right breast, indicating a suspicious mass, adjacent to this lesion, a cystic area with echogenic contents was observed, suggesting a possible necrotic component. Enlarged right axillary lymph nodes were also noted, suggestive of nodal metastasis. No significant abnormalities were detected in the left breast, and the left axillary lymph nodes appeared benign. These findings were categorized as BIRADS-5, and a biopsy was advised for further evaluation. CECT (Contrast Enhanced Computed Tomography) showed a well-defined irregular heterogeneously enhancing mass in the upper quadrant of the right breast with involvement of the nipple-areola-complex, skin and right axillary lymph nodes. A trucut biopsy of the right breast lump revealed features consistent with invasive ductal carcinoma of no special type, Grade III (score 8). Immunohistochemistry results showed ER-negative, PR-negative, HER2neu-negative, Ki67 at 80%, and negative staining for Synaptophysin and CD56. A PET (Positron Emission Tomography) scan revealed a metabolically active mass in the supralateral quadrant of the right breast measuring 70×7.05×85 mm, along with an enlarged and metabolically active right level I axillary lymph node measuring 20.5×24 mm with no other distant metastases noted. The patient was diagnosed with Metastatic Carcinoma Breast cT4b N2a M1 and received palliative chemotherapy after Cardiac clearance, Liver Function Tests, and Renal Function Tests evaluation, consisting of 6 cycles of Paclitaxel and Carboplatin. There was partial response post-chemotherapy. She underwent a palliative mastectomy, followed by 6 cycles of adjuvant chemotherapy with Capecitabine.
After a month, she presented with complaints of diplopia, occipital throbbing headache radiating to the temporal region and non-bilious projectile vomiting. MRI (Magnetic Resonance Imaging) of the Brain revealed left temporal lobe (1.7×2.3 cm) and right occipital (1.75×1.74 cm) metastases with surrounding brain oedema with a midline shift of 3 mm at the level of Foramen of Munro as depicted in (Figure 1). She received wholebrain radiotherapy followed by palliative chemotherapy with three weekly Docetaxel 75 mg/m2 with appropriate pre-medication & post-medication, using Dexamethasone, Ranitidine and Ondansetron. Supportive treatment with corticosteroids, osmotic diuretics and anti-hypertensives was also given. After 5 days of the first cycle of Docetaxel 108 mg, she presented to casualty with sudden onset breathlessness-Grade 4 mMRC and dry cough. On auscultation, reduced breath sounds over the right upper and mid zones with early inspiratory crackles were noted. ECG (Electrocardiogram) and 2D-Echocardiography were normal. Blood investigations revealed a normal leukocyte count with high CRP (C-Reactive Protein) and ESR (Erythrocyte Sedimentation Rate). Serum procalcitonin and D-dimer were normal. USG (Ultrasonogram) of Thorax revealed no evidence of pleural effusion. CTPA (Computed Tomography Pulmonary Angiography) revealed no evidence of pulmonary embolus. RT-PCR and BAL for microbiological assay were negative. HRCT (High Resolution Computed Tomography) of Thorax revealed diffuse homogenous and non-homogenous ground-glass opacities suggestive of drug-induced interstitial pneumonitis, as noted in (Figure 2). The patient’s respiratory status deteriorated rapidly, requiring intubation and empirical therapy with intravenous antibiotics. The patient was started on intravenous methylprednisolone. Despite supportive measures, the patient succumbed to Type-2 respiratory failure and expired. Post mortem biopsy of the lung was done, and acute interstitial pneumonitis was confirmed, as seen in (Figure 3).
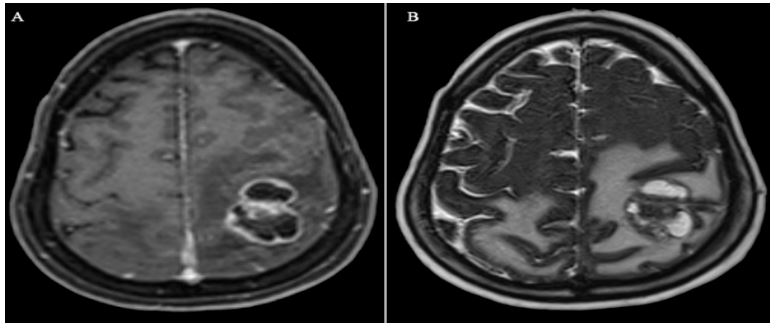
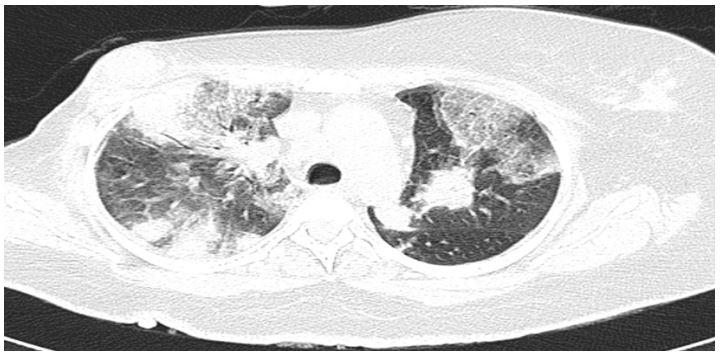
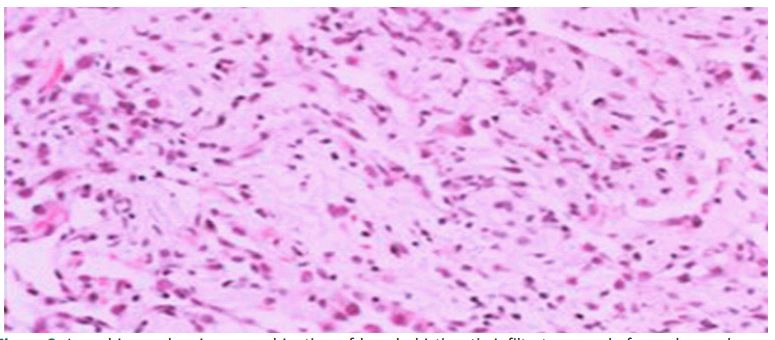
Table 1: Laboratory parameters of the patient, along with normal reference range.
| Parameter | Value | Normal reference range |
|---|---|---|
| Serum C-Reactive Protein (CRP) | 0.43 mg/dL | <1 mg/dL |
| Erythrocyte Sedimentation Rate (ESR) | 4 mm/hr | <20 mm hr |
| Serum Procalcitonin | 0.013 ng/mL | <0.1 ng/mL |
| Serum D-dimer | 0.06 mg/L | <0.5 mg/L |
| Hemoglobin | 10.6 mg/dL | 10.5-13.5 mg/dL |
| Total Leukocyte Count | 9,400/cm3 | 4000-11,000/cm3 |
| Platelet Count | 2.8 lakh/µL | 1.5-4.5 lakh/µL |
Discussion
Docetaxel-induced interstitial pneumonitis is a serious and potentially life-threatening complication that, although uncommon, carries a high mortality rate [9]. As described in previous case reports, such as those by Ochoa et al. (2012) and Nagata et al. (2010), pneumonitis typically presents after the administration of Docetaxel, often within two cycles of standard dosing [9,10]. In our case, the patient developed interstitial pneumonitis after the first cycle of Docetaxel (75 mg/m²), which is consistent with the timeline reported in the literature but highlights the potential for this adverse event to occur even earlier. As noted by Pankowska-Supryn et al. (2015), the diagnosis is primarily based on clinical and radiological findings, supported by the exclusion of other possible causes such as opportunistic infections, pulmonary embolism, and lymphangitic carcinomatosis [7]. In our patient, these differential diagnoses were carefully ruled out through extensive workup, including negative RT-PCR (Real-time Reverse Transcription-Polymerase Chain Reaction) and BAL (Bronchoalveolar Lavage) for microbiological assays, normal CTPA, and USG Thorax findings. HRCT-Thorax was instrumental in identifying the diffuse ground-glass opacities characteristic of interstitial pneumonitis. The exact mechanism of lung injury is debatable, the most common pattern of lung injury described is that of hypersensitivity pneumonitis [7]. Taxanes are known to stimulate cytotoxic T-cell proliferation, which can lead to hypersensitivity-type lung injury or direct pulmonary dam-age through reactive oxygen metabolites [11]. The incidence of pulmonary toxicity appears to be more closely related to the docetaxel delivery schedule rather than the dosage, with weekly administration associated with higher rates of pneumonitis but lower myelosuppression compared to a triweekly regimen [12]. In our case, the standard triweekly regimen was used, yet the patient developed severe pneumonitis, suggesting that even conventional dosing schedules carry significant risks. Prompt recognition and treatment of taxane-induced pneumonitis are critical for patient survival. As highlighted in the case series by Bielopolski et al. (2017), rapid initiation of high-dose corticosteroids is essential in managing this condition, as pulmonary toxicity can be reversed with timely intervention [13]. Despite initiating intravenous methylprednisolone in our patient, the severity of the pneumonitis led to rapid respiratory deterioration, ultimately resulting in type-2 respiratory failure and death. This outcome underscores the aggressive nature of docetaxel-induced pneumonitis and the importance of early diagnosis and treatment.
Conclusion
Our case report contributes to the growing body of literature on docetaxel-induced interstitial pneumonitis by reinforcing the need for vigilance in monitoring patients receiving taxane-based chemotherapy. Early identification, multidisciplinary evaluation, and immediate intervention are paramount in mitigating the risks of this potentially fatal complication and preventing mortality. Furthermore, ongoing research into the mechanisms underlying taxane-induced pulmonary toxicity is necessary to understand better and mitigate these risks.
Declarations
Acknowledgments: The authors would like to thank the patient and their family for their cooperation and willingness to contribute to medical knowledge through this case report. We also extend our gratitude to the medical and nursing staff involved in the patient’s care for their dedication and support.
Statement of ethics: This case report was reviewed and approved by the Institutional Ethics Committee. Since this is a case report, formal ethical approval was not required according to the committee’s guidelines.
Written informed consent for publication of case: Written informed consent was obtained from the patient’s next-of-kin for the publication of this case report, including the associated clinical details and accompanying images.
Conflict of interest statement: The authors declare that they have no conflicts of interest to disclose.
Funding sources: This study was not supported by any sponsor or funder.
Author contributions: Dr. Bana Mary Manishaa: Conceptualization, clinical case handling, and manuscript writing. Dr. Bhargav Shreeram Gundapuneedi: Data collection, interpretation, radiotherapy planning, chemotherapy treatment and manuscript revision. All authors have read and agreed to the final manuscript.
Data availability statement: The data supporting the findings of this case report are not publicly available due to the sensitive nature of patient information, but are available from the corresponding author [Dr. Bana Mary Manishaa; Email-banamary. manishaa@student.sbvu.ac.in] upon reasonable request under ethical and legal guidelines.
References
- Anoop T, Joseph R, Unnikrishnan P, Thomas F, Venugopal M: Taxane-induced acute interstitial pneumonitis in patients with breast cancer and outcome of taxane rechallenge. Lung India. 2022; 39: 158.
- Bouros D, Nicholson AC, Polychronopoulos V, Du Bois RM: Acute interstitial pneumonia. Eur Respir J. 2000; 15: 412.
- Manuprasad A, Ganesan P, Mahajan V, Ganesan TS, Radhakrishnan V, Dhanushkodi M, et al. Docetaxel-Induced Lung Injury: An Under-Recognized Complication of a Commonly Used Chemotherapeutic Agent. Indian Journal of Medical and Paediatric Oncology. 2019; 40: 208–11.
- Michaud LB, Valero V, Hortobagyi G. Risks and Benefits of Taxanes in Breast and Ovarian Cancer: Drug Safety. 2000; 23: 401– 28.
- Ostoros G, Pretz A, Fillinger J, Soltesz I, Dome B: Fatal pulmonary fibrosis induced by paclitaxel: a case report and review of the literature. International Journal of Gynecological Cancer. 2006; 16: 391–3.
- Fujimoto D, Kato R, Morimoto T, et al. Characteristics and Prognostic Impact of Pneumonitis during Systemic Anti-Cancer Therapy in Patients with Advanced Non-Small-Cell Lung Cancer. PLoS ONE. 2016; 11: e0168465.
- Pankowska-Supryn M, Załęska M, Roszkowska-Śliż B, RoszkowskiŚliż K. Interstitial Lung Disease Associated with Docetaxel in a Patient Treated for Breast Cancer—A Case Report. Advances in Respiratory Medicine. 2015; 83: 378–82.
- Min B-D, Kang H-W, Kim W-T, Kim Y-J, Yun SJ, Lee SC, Kim W-J: Docetaxel-Induced Fatal Interstitial Pneumonitis in a Patient with Castration-Resistant Prostate Cancer. Korean J Urol. 2012; 53: 371.
- Ochoa R, Bejarano PA, Glück S, Montero AJ. Pneumonitis and pulmonary fibrosis in a patient receiving adjuvant Docetaxel and cyclophosphamide for stage 3 breast cancer: a case report and literature review. J Med Case Reports. 2012; 6: 413.
- Nagata S, Maehara Y, Nagata S, Ueda N, Yoshida Y, Matsuda H, et al. Severe interstitial pneumonitis associated with the administration of taxanes. Journal of Infection and Chemotherapy. 2010; 16: 340–4.
- Chang CY, Wang CJ, Chang HT. Docetaxel-related interstitial pneumonitis. TCRM. 2015: 1813.
- Raghupathi R, Patil C, Dhiman P: Drug-induced infiltrative lung disease with weekly paclitaxel in breast cancer: Case series. J Can Res Ther. 2021; 17: 262.
- Bielopolski D, Evron E, Moreh-Rahav O, Landes M, Stemmer SM, Salamon F: Paclitaxel-induced pneumonitis in patients with breast cancer: case series and review of the literature. Journal of Chemotherapy. 2017; 29: 113–7.