
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
MDS-Cutis in a patient with myelodysplastic syndrome treated with Azacitidine, heralding progression to acute leukaemia
Alice Cassie1 ; Gehad Elgabry2 ; Madhavi Maheshwari3 ; Judith Caddick4 ; Farooq Wandroo2 *
1Department of Haematology, University Hospital Birmingham, UK.
2Department of Haematology, Midland Metropolitan University Hospital Health Campus, Sandwell and West Birmingham Hospitals NHS Trust, Birmingham,UK.
3Black Country Pathology Network, New Cross Hospital, The Royal Wolverhampton NHS Trust, UK.
4West Midlands Genomics Laboratory, Birmingham Women’s and Children’s NHS Foundation Trust, Birmingham, UK.
*Corresponding Author : Farooq A Wandroo, MD, FRCP, FRCPath, FRCpathME
Honorary Associate Professor, University of Birmingham,
Consultant Haematologist, Department of Haematology,
Midland Metropolitan University Hospital, SWBH NHS
Trust, Grove Lane Smethwick, Birmingham, B662QT, UK.
Email: Farooq.wandroo@nhs.net
Received : Jan 13, 2025
Accepted : Feb 28, 2025
Published : Mar 07, 2025
Archived : www.jcimcr.org
Copyright : © Wandroo FA (2025).
Citation: Cassie A, Elgabry G, Maheshwari M, Caddick J, Wandroo F. MDS-Cutis in a patient with myelodysplastic syndrome treated with azacitidine, heralding progression to acute leukaemia. J Clin Images Med Case Rep. 2025; 6(3): 3499.
Introduction
There are a wide range of dermatological presentations seen in haemato-oncology patients. Correctly identifying and diagnosing skin pathology can be additionally complex, as cutaneous reactions can be secondary to an immunocompromised state, exposure to a wide range of drugs including chemotherapy agents, or an infiltration of an underlying malignancy.
Myelodysplastic syndrome (MDS) has several associated skin pathologies varying from neutrophilic dermatoses, vasculitis (particularly leukocytoclastic vasculitis) and leukaemia cutis. This is in addition to the more commonly seen drug reactions, viral and bacterial infections and other autoimmune associated skin conditions.
Neutrophilic dermatoses are a group of disorders including several entities such as Sweet syndrome and pyoderma gangrenosum , which have histopathological features of neutrophilic infiltration in cutaneous tissues. Classical Sweet syndrome (SS) is associated with malignancy (particularly haematological malignancy) but majority of cases have non-malignant associations like drug, infections or autoimmune base. A variant of Sweet syndrome called Histiocytoid Sweet syndrome (H-SS) has been more closely linked with MDS than the classical subtype, although many are also associated with non-malignant causes and histological features show dermal infiltrates of cells with a myeloid lineage.
Additionally, cutaneous manifestations of haematological malignancies can also be rarer forms of skin pathology. Leukaemia cutis, described as infiltration of malignant leukocytes or blasts into the skin, has most often been recognised in particular association with Acute Myeloid Leukaemia (AML). It can however be seen in other leukaemia’s andeven as a precursor in MDS prior to transformation in the bone marrow, it has been suggested to be a poor prognostic marker in all groups of affected patients.
More recently, literature has suggested a newer entity in MDS with similar features to both Sweet syndrome (specifically the Histocytoid subset) and Leukaemia cutis [1]. Histology in these cases shows histocytoid infiltration as is typical of H-SS but additionally with immunophenotyping and cytogenetics proving the cutaneous lesions to be clonally in keeping with bone marrow and peripheral blood pathology. Lesions in these cases have been subsequently described as Myelodysplastic Cutis (MDS-Cutis) [6-8]. It is important to note that MDS-Cutis is only associated with MDS and often heralds transformation to acute leukaemia.
These uncommon and complex presentations present an interesting diagnostic challenge in haematology patients, encouraging us to look beyond the clinical presentation in the skin itself to consider the wider histology and even genetics of such lesions. Recognising MDS-Cutis as a separate entity could lead to more targeted investigations and treatments in such patients.
Case presentation
Investigations/results
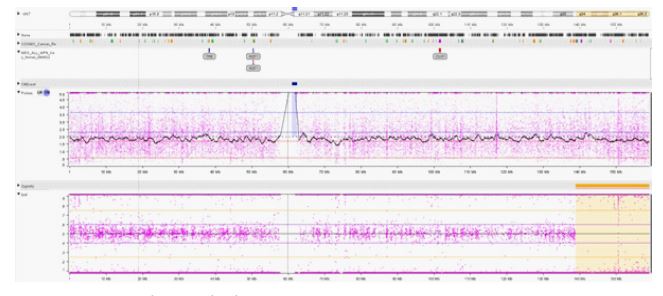
This is the presentation of a 78-year-old Afro-Caribbean male patient with a background of previous prostate cancer (treated and in remission), Osteoarthritis of the spine, Type 2 Diabetes mellitus, irritable bowel syndrome and gout. He first presented to haematology with a new pancytopenia in May 2022 which was subsequently diagnosed as high risk MDS. Aspirate results showed about 5% myeloblasts with dysplastic features in all cell lines. Bone marrow trephine results suggested a blast excess of 5-10% which were positive for CD34, CD117, and CD15 on immunohistochemical stains. Single nucleotide polymorphism (SNP) array analysis of the bone marrow confirmed abnormal clones with tetrasomy 8 and copy neutral loss of heterozygosity (CN-LOH 7q) (Figure 7,8). Next Generation Sequencing (NGS) showed a number of mutations of clinical significance like U2AF1, ASXL1, SETBP1 and GATA2. His IPSS-R Score was calculated at 6. He was treated with subcutaneous Azacitidine as a first line treatment.
Following the first cycle of Azacitidine S/C 65 mg × 2 doses, erythematous tender areas began to appear at the patient’s injection sites. After further swelling to the affected areas and increasing discomfort, for an abdominal wall ultrasound showed only extensive thickening of anterior abdominal fat.
Whilst this was initially seen as reassuring about twelve days later he went on to develop new nodular lesions on his face and scalp with associated temperatures (Figure 1). The lesions began to increase in size and number across the face, scalp and abdomen. They were predominantly rounded popular lesions, of which some had started to ulcerate and crust, with necrotic changes seen on lesions to the cheek lesions bilaterally. Biopsies were sent and he was started on oral prednisolone 70 milligrams daily.
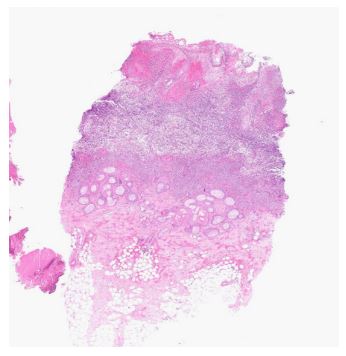
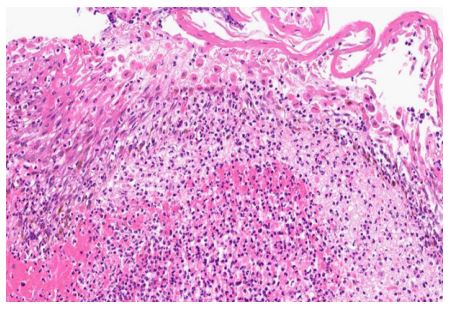
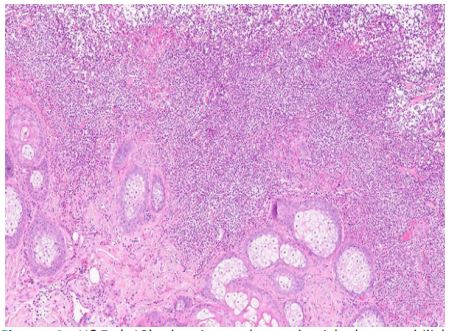
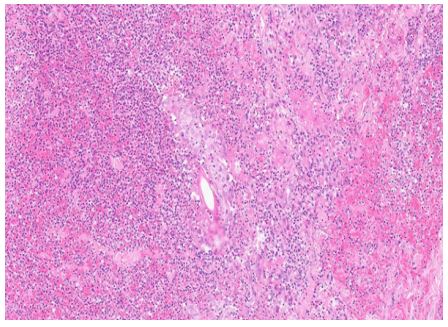
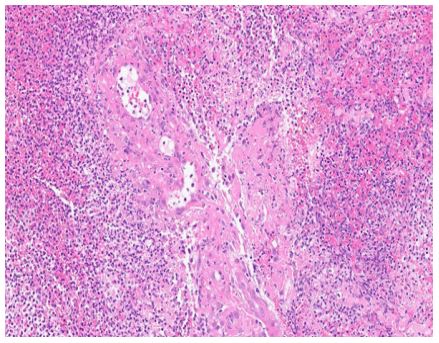
Initial histology results were taken from two biopsies, one from an abdominal lesion (Figure 2) and another from a facial lesion from the right cheek (Figures 3-6). Both biopsies were similar on examination, with epidermal ulceration and predominantly neutrophilic infiltration in the superficial and mid dermis. No atypical haematolymphoid cells were identified. The histopathology was reported as in keeping with neutrophilic dermatoses, most likely to be representative of a Sweet syndrome or pyoderma gangreosum.
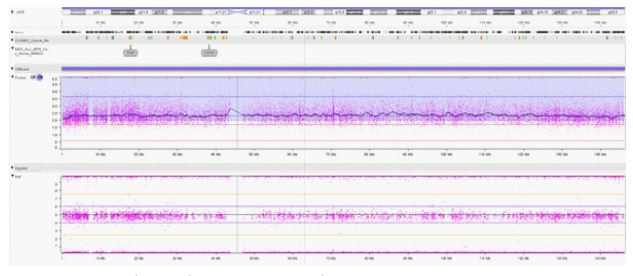
Genetic analysis of the skin lesions revealed the same clinically significant same variants in U2AF1, ASXL1, SETBP1 and GATA2 in tissue biopsy as seen in marrow. Importantly, the same abnormal clone with CN-LOH 7q from previous bone marrow results were seen (Figures 9,10).
Differential diagnoses
The initial presentation of this case was highly suggestive of a neutrophilic dermatosis and in particular Sweet syndrome. The clinical picture of new popular and nodular lesions with elements of ulceration and necrosis with associated fevers supported the diagnosis of SS. The causative agent was felt to be the patient’s underlying diagnosis of MDS, or potentially a drug they had been exposed to during his treatment such as Azacitidine. It was not until cytogenetic correlation that these lesions were considered to be distinct entity of Myelodysplastic syndrome cutis (MDS-Cutis).

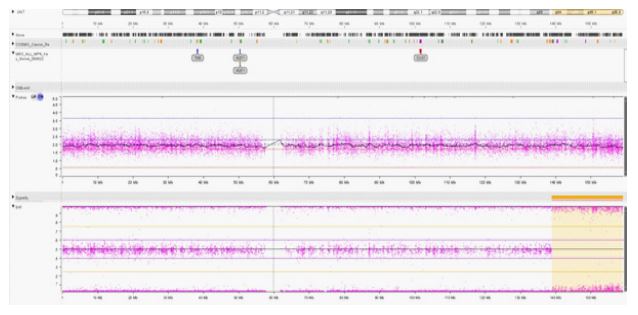
SNP array analysis on Bone marrow: Chromosome 7; 20 Mb CN-LOH 7q34 - qter ~90% cells (estimate).
SNP array analysis on bone marrow: Chromosome 8; Clear copy number (CN) gain, without loss of heterozygosity, consistent with with tetrasomy 8 in 16% cells.
SNP array analysis on skin lesion: Chromosome 7; 20 Mb CN-LOH 7q34- qter ~90% cells (estimate).
Discussion
This case report is about this relatively new entity of Sweet syndrome (SS) called MDS-Cutis. The clinical and histological findings of Sweets syndrome, MDS-Cutis and Leukaemia cutis can have similar clinical presentations and findings. These uncommon cutaneous reactions may be a known association in haematological malignancy and/or with some associated chemotherapy agents but remain poorly understood and is a subject of ongoing investigation and research [9]. The SS is categorised into classic SS and drug induced SS (DI-SS), together these constitute 80% of SS cases. Malignancy associated SS (MA-SS) constitute only 20% of SS cases, and a large majority of these are due to MDS and acute myeloid leukaemia (AML) [21].
Classical Sweet syndrome and the Histiocytoid variant have been associated in MDS in a number of case series and reviews [10,11], but Classic Sweet syndrome is more often associated with non-malignant conditions like viral/bacterial infections, autoimmune conditions and numerous drugs (antibiotics, antiinfammtory, anti neoplastic drugs, growth factors and antiepileptics) [22] when compared with Histiocytoid variant. Typical treatment for suspected and confirmed Sweet syndrome is with systemic corticosteroids [12] as was given to our patient when sweets syndrome was initially suspected. Steroid treatment has been shown to lead to complete response in many cases and resolution without relapses following an acute presentation of symptoms in classical sweet syndrome overall [13].
In cases with Sweet syndrome related to a causative drug agent [14], withdrawal of the implicated drug has shown spontaneous resolution. Additionally, Sweet and H-SS secondary to underlying malignancy (or those of the classical type following a chronic relapsing course) such as MDS have been shown to resolve with hypomethylating agents targeting the underlying malignancy including agents such as Azacitidine [15].
The initial difficulty in our case was first distinguishing the likelihood of Azacitidine either precipitating the symptoms or whether it was coincidental with the underlying MDS. Several case studies have previously highlighted Azacitidine as a cause of Sweet syndrome [16]. In contrast to this, there are additional cases showing Azacitidine as an effective treatment in Sweet syndrome in patients with underlying MDS [17], complicating an already challenging diagnosis. The timeline we have presented clearly shows a correlation between Azacitidine therapy and symptoms, although reports linking Azacitidine to Sweet syndrome have a quicker onset of symptoms such as within 3-5 days [18] which was not seen for our patient. The start of treatment to time of skin symptom onset was slightly longer at 12 days. The resolution of the cutaneous symptoms was observed in these similar cases with withdrawal of Azacitidine and commencing steroid treatment. Whilst the hand and face lesions of our case resolved over the next month, the abdominal lesions remained ulcerated and erythematous lesions stayed for several months after the initial presentation, although static and non-progressing in appearance.
We could not re-challenge the patient with Azacitidine fearing flare up of his MDS-Cutis. His WBC count remained at 30- 40000x109 /dl for several months after the resolution of his skin lesions. Six months later he finally transformed to acute leukaemia and died due to his disease.
It was not until histology results of the lesion were incorporated with the cytogenetic and molecular analysis (SNP array and NGS analysis) that MDS-Cutis was realised as a distinct possibility. As previously mentioned, the recognition of MDS-Cutis as a separate diagnostic entity has been new over the past few years. Generally described as between the spectrum of disorders between H-SS and Leukaemia cutis it is diagnosed only with the clonally related myeloid cells being present in the bone marrow and skin lesions, [19] as was evidenced in the results of our case.
The significance of MDS-Cutis being a distinct diagnosis casts doubt in regards to how this should guide treatment options. Whilst it is suggested that hypomethylating agents and MDS targeted treatments may have a more beneficial role than steroids there is not a enough evidence to currently support this. The role of drugs such as Azacitidine remains particularly complicated given the possibility of Sweets like reactions from the drug itself even noting the rarity of reported case studies. However, MDS-Cutis is always associated with MDS unlike classic Sweet which has wide underlying aetiology.
Whilst Sweet syndrome and its variants are often highly treatable, at the other end of this spectrum leukaemia cutis has a very poor prognosis. Leukaemia cutis is more often recognised in underling acute leukaemia’s such as acute myeloid leukaemia (AML) but can be seen in cases of MDS before bone marrow and peripheral blood transformation. That is exactly what we saw in our case who finally transformed to AML within 6 months of the diagnosis of MDS- Cutis. Therefore, the diagnosis can have a significant impact on treatment and outlook for patients which shouldn’t be overlooked. The prognosis and outlook for MDSCutis is variable but remains linked in case studies to more highrisk variants of the disease as seen in our case report.
Whilst we need to learn to explore further treatments for MDS-Cutis, the role of molecular and cytogenetic testing in such patients has clearly broadened the ability for more specific diagnosis which may lead to AML like treatment and more targeted treatments in future if a marker is identified.
Learning points
1. Cutaneous pathologies in haematooncology patients are common and varied.
2. Presentations may have similar clinical and histological findings but molecular and cytogenetic testing may aid diagnosis and allow for targeted treatments.
3. MDS-Cutis should be considered when investigating cutaneous pathology inpatients with an MDS diagnosis. It is worth performing extensive SNP and NGS analysis of the tissue specimen.
4. Cutaneous pathology with associated molecular changes can be relevant as a prognostic marker and can be an early sign of transformation to AML. Hence this will aid in choosing AML directed therapy.
References
- Wallach D, Vignon-Pennamen M-D. Pyoderma gangrenosum and Sweet Syndrome: The prototypic neutrophilic dermatoses. British Journal of Dermatology. 2015; 178: 595–602.
- Sweet RD. An acute febrile Neutrophilic dermatosis. Br J Dermatol. 1964; 76: 349-56.
- Ferea CR, Mihai SN, Balan G, Badescu MC, Tutunaru D, Tatu AL. Sweet Syndrome Associated with Myelodysplastic Syndrome— A Review of a Multidisciplinary Approach. Life. 2023; 13: 809.
- Paydas¸ S, Zorludemir S. Leukaemia Cutis and Leukaemic Vasculitis. British Journal of Dermatology. 2000; 143: 773–9.
- Findakly D. Leukemia cutis: A systematic review. Blood. 2020; 136: 1–1.
- Delaleu J, Battistella M, Rathana K, Vignon‐Pennamen MD, Laurent C, Ram‐Wolff C, et al. Identification of clonal skin myeloid cells by next‐generation sequencing in Myelodysplasia Cutis. British Journal of Dermatology. 2020; 184: 367–9.
- Calvo KR. Skin in the game: The Emergence of Myelodysplasia Cutis. Blood. 2022; 139: 1132–4.
- Delaleu J, Kim R, Zhao LP, de Masson A, Vignon-Pennamen MD, Cassius C, et al. Clinical, pathological, and molecular features of Myelodysplasia Cutis. Blood. 2022; 139: 1251–3.
- Ferea CR, Mihai SN, Balan G, Badescu MC, Tutunaru D, Tatu AL. Sweet syndrome associated with myelodysplastic syndrome—a review of a multidisciplinary approach. Life. 2023; 13: 809.
- Dev T, Agarwal S, Khandpur S. Histiocytoid Sweet Syndrome: A rare variant of classic paraneoplastic derm tosis in relation to myelodysplastic syndrome - A case report. Indian Journal of Medical and Paediatric Oncology. 2020; 41: 748–51.
- Ghoufi L, Ortonne N, Ingen‑Housz‑Oro S, Barhoumi W, Begon E, Haioun C, et al. Histiocytoid sweet syndrome is more frequently associated with myelodysplastic syndromes than the classical neutrophilic variant: A comparative series of 62 patients. Medicine (Baltimore). 2016; 95: e3033
- Cohen PR, Kurzrock R. Sweet’s syndrome: a review of current treatment options. Am J Clin Dermatol. 2002; 3: 117-31.
- Sweet Syndrome: Clinical presentation, associations, and response to treatment in 21 patients. Journal of the American Academy of Dermatology. 2015; 72.
- Cohen, P.R., Kurzrock, R. Sweet’s Syndrome. Am J Clin Dermatol. 2002; 3: 117–131.
- K Raj, A Ho, JD Creamer, AWP Du Vivier, JR Salisbury, GJ Mufti, et al. Complete response of deep neutrophilic dermatosis associated with myelodysplastic syndrome to 5‐azacytidine, British Journal of Dermatology. 2007; 156: 1039–1041.
- Bonazza S, Dalton B, Hardin J, Metelitsa A. Histiocytoid variant of sweet syndrome associated with Azacitidine and recurrence upon rechallenge. Can J Hosp Pharm. 2015; 68: 339-41.
- Martinelli S, Rigolin GM, Leo G, Gafà R, Lista E, Cibien F, et al. Complete remission of Sweet’s syndrome after azacytidine treatment for concomitant myelodysplastic syndrome. Int J Hematol. 2014; 99: 663-7.
- Hannah B. Trickett, Aaron Cumpston, Michael Craig, Azacitidineassociated Sweet’s syndrome, American Journal of Health-System Pharmacy. 2012; 69: 869–871.
- Calvo KR. Skin in the game: The Emergence of Myelodysplasia Cutis. Blood. 2022; 139: 1132–4.
- Merlant, M.; Lepelletier, C.; Battistella, M.; Vignon-Pennamen, M.-D.; Duriez, P.; Moguelet, P.; Brunet-Possenti, F.; Bagot, M.; Chasset, F.; Bouaziz, J.D. Acute myeloid leukemia and myelodysplastic syndrome–associated Sweet syndrome: A comparative multicenter retrospective study of 39 patients. J Am Acad Dermatol. 2020; 84: 838-840.
- Cohen, P.R. Sweet’s syndrome—A comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007; 2: 34.
- Vignon-Pennamen, M.D.; Osio, A.; Battistella, M. Histiocytoid Sweet Syndrome and Myelodysplastic Syndrome. JAMA Dermatol. 2017; 153: 835-836.