
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
A rare case of primary amenorrhea with Swyer syndrome: A case report
*Corresponding Author : Ashwini H
Hull York Medical School, York Biomedical Research
Institute, University of York, York, UK.
Email: ashwijay85@gmail.com
Received : Feb 03, 2025
Accepted : Mar 03, 2025
Published : Mar 10, 2025
Archived : www.jcimcr.org
Copyright : © Ashwini H (2025).
Abstract
Background: Swyer syndrome is seen in females with primary amenorrhea, unambiguous female genital appearance, normal vagina and cervix but XY karyotype. It is characterized by bilateral streaky ovaries, hypoplastic infantile uterus, normally developed Mullerian structures, hypergonadotropic hypogonadism. The incidence of swyer syndrome is about one in 80,000. It is a rare genetic condition affecting sexual organ development, classified as Disorder of Sex Development (DSD). Affected individuals usually have a uterus and fallopian tubes, but their gonads are not functional. Instead, the gonads are small and underdeveloped and contain little gonadal tissue.
Case presentation: Family history and the age at diagnosis was collected. Physical examination for secondary sexual characteristics was done. Initial laboratory tests for evaluating Primary amenorrhoea like TSH, FSH & Esteriole were done. Radiodiagnosis to find uterine & ovaries size. Karyotyping and FISH tests were done to find the genotype of the girl.
Conclusion: A 17 year old unmarried girl was born to second degree consanguineous parents. She measured 167 cm tall and weighed 44 kg. On examination, breasts were in tanner stage 2, with absent axillary hair but well developed pubic hair, healthy vagina & small cervix. External genitalia was of female type.
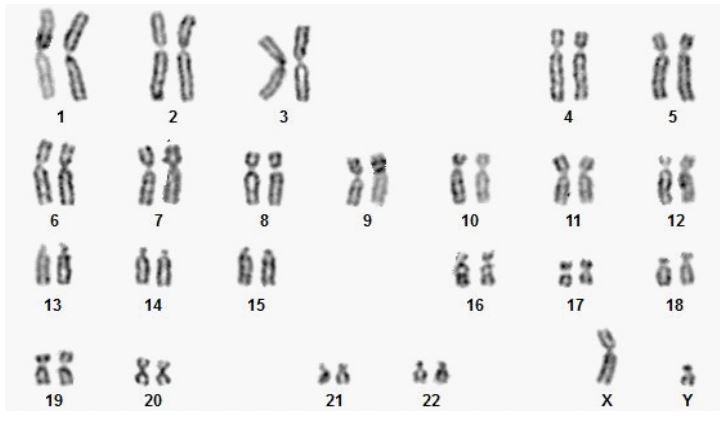
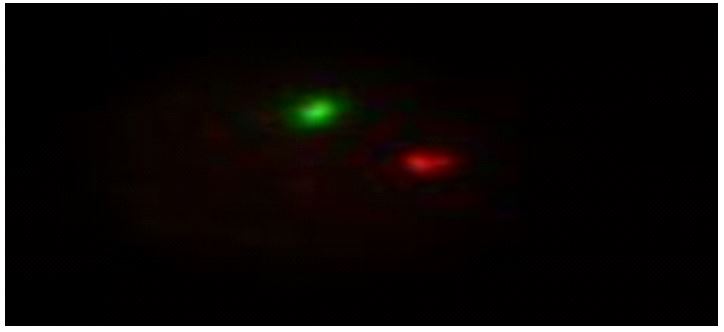
Laboratory tests showed: FSH-47.316, LH-34.986, Estradiol-66.969 MRI revealed hypoplastic infantile uterus, bilateral streaky ovaries. Karyotype analysis showed 46XY karyogram. FISH test showed signals for one X and one Y chromosomes and no mosaic pattern for sex chromosomes was seen.
Keywords: Primary amenorrhea; Swyer syndrome; Hypogonadism; 46XY female.
Citation: Ashwini H. A rare case of primary amenorrhea with Swyer syndrome: A case report. J Clin Images Med Case Rep. 2025; 6(3): 3502.
Introduction
Swyer syndrome or pure 46XY gonadal dysgenesis is a condition in which the individuals have female appearance [1]. They classically present as sexually infantile phenotypic females with primary amenorrhoea. People with this disorder have female external genitalia but the uterus and fallopian tubes are underdeveloped. However, they do not have functional gonads (ovaries or testes). Instead, they have streak gonads [1].
Complete gonadal dysgenesis or Swyer syndrome was first described by Jim Swyer in 1955; since then, a number of cases were reported [2]. It is characterized by bilateral streak gonads, normally developed Mullerian structures, female‑appearing external genitalia, and hypergonadotropic hypogonadism [2]. Patients usually present in adolescence with primary amenorrhea and with lack of secondary sexual characteristics. The incidence of Swyer syndrome is 1:80,000 [3]. The purpose of reporting this case is its rarity and the importance of diagnosis of XY female for appropriate management as there is a high incidence of gonadal malignancies and also to counsel about fertility options.
A small number of successful pregnancies achieved with oocyte donation have been reported in patients with Swyer syndrome [3].
Case presentation
A 17-year-old female patient (Figure 1) sought medical attention at S Nijalingappa Medical College and HSK Hospital in Bagalkote, Karnataka, India, due to the absence of menstruation. The patient had no notable surgical background. She reported no recurring abdominal discomfort, exposure to hormones or radiation, or neurological symptoms like headaches or vision problems. She was the eldest child of parents who were second-degree relatives. Her younger sibling was a healthy male. Physical assessment revealed her height as 167 cm and a body mass index of 15.8 kg/m2 . Evaluation of her sexual development showed Tanner stage 2 breast growth, underdeveloped secondary sexual characteristics (bilateral Streeky ovary), lack of axillary hair, and well-formed pubic hair.
Inspection of the external genitalia indicated female characteristics, with a visible vaginal opening. Subsequent tests revealed elevated serum hormone levels: follicle-stimulating hormone at 47.3 mIU/L and luteinizing hormone at 34.96 mIU/L. Estradiol was measured at 66.969 mIU/L. Imaging studies showed abnormal reproductive organs: ultrasound detected a rudimentary uterus (Figure 2), while magnetic resonance imaging revealed an underdeveloped uterus lacking fallopian tubes and with streak-like ovaries, without distinct endometrial or myometrial layers. Both kidneys appeared normal. Genetic analysis through karyotyping (Figure 3) identified a 46XY genotype. To validate this finding and rule out potential false results, Fluorescent In situ Hybridization (Figure 4) was conducted, which confirmed the presence of one X and one Y chromosome in all examined cells.


Discussion
Swyer syndrome affects individuals with XY chromosomal make-up; nevertheless they have a female appearance. The exact incidence is unknown. It has been estimated to occur in 1 in 80,000 births. The diagnosis of Swyer syndrome is made based on thorough clinical evaluation, detailed patient history, identification of characteristic findings (e.g., amenorrhoea and streak gonads), and a variety of tests including karyotyping and FISH. The height of the patient is particularly helpful in distinguishing patients with pure 46XY gonadal dysgenesis from those with 45XO/46XY mosaicism but without the classic features of Turner syndrome [4]. The chromosomal analysis in Swyer syndrome shows a male karyotype (46XY) and FISH signals for male.
This case showed that the diagnosis was in time and done only at the age of 17 years. A study by Michala et al. [3] also shows that many women experienced delay in reaching accurate diagnosis, often several years after the presentation to their general practitioners. It is suggested that health professionals should update their scientific knowledge and be aware of sexual development disorders. Early diagnosis is important for a number of reasons: firstly, because of the risk of gonadal malignancy; secondly, early institution of hormonal therapy is vital for the induction of puberty; thirdly, HRT is required to prevent osteoporosis [1]. The risk of tumour development in Swyer syndrome is significant. A 20% to 30% incidence of tumour in Swyer syndrome was reported [4]. The most common tumour involved in this condition is gonadoblastoma [2]. Dysgerminoma and embryonal carcinoma were also reported [2]. Due to the risk of tumours, extensive search for the rudimentary gonads is needed and bilateral gonadectomy is advisable. As for this patient, since we could not detect any rudimentary gonads, she requires a close follow-up in the long run. An interesting finding in this patient is that despite late induction of puberty and non-compliance to hormonal treatment, there is marked improvement in her uterine development. However, her uterine size was small than in normal controls. This finding was similar to the study carried out by [3] the small uterine size however did not appear to have adverse effect on the fertility outcome in Swyer syndrome [2]. A small number of successful pregnancies have been reported in this group of patients [1,3]. Pregnancies were possible through oocyte donation and hormonal treatment. The presence of the XY genotype and the H-Y antigen does not affect the normal uterine and endometrial response. Thus, the possibility of maintaining normal pregnancy and delivery confirms the physiological ability of the uterus to accommodate and maintain successful pregnancy in patients with XY dysgenesis [5].
Conclusion
Swyer syndrome is extremely rare and invariably causes primary amenorrhea. Genetic testing plays very important role in the diagnosis of Swyer syndrome. Early diagnosis is of crucial importance for various reasons, including the risk of gonadal malignancy and the need for removal of the gonads, early institution of HRT for induction of puberty, improving bone mineral density, and also counseling regarding fertility options.
Declarations: I declare that the submitted case paper is my original work and no part of it has been published any were else in the past. I take full responsibility, that if in future, the paper is found invalid according to basic rules, the last decision will be of the authorities concern.
References
- Negar K, Saber G, Mahdi E. Swyer syndrome in a woman with pure 46,XY gonadal dysgenesis and a hypoplastic uterus: a rare presentation. Fertil Steril. 2010; 93: 1. Doi:10.1016/j. fertnstert.2009.09.062.
- Granados H, Phulwani P. Absent visualization of a hypoplastic uterus in a 16 year old with complete 46 XY gonadal dysgenesis (swyer syndrome). Endocrinol Metab Syndr 2013; 2: 1143.
- Michala L, Goswami D, Creighton SM, et al. Swyer syndrome: presentation and outcomes. BJOG 2008; 115: 737-41.
- Nadereh B, Mojgan KZ. Dysgerminoma in three patients with Swyer syndrome. World J Surg Oncol 2007; 5: 71. Doi: 10.1186/1477-7819-5-71.
- Babre VM, Bendre K, Niyogi G. A rare case of swyer syndrome. Int J Reprod Contracept Obstet Gynecol 2013; 2: 485-7.