
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Review Article - Open Access, Volume 6
How I treat my patients with Myalgic Encephalomyelitis, Chronic Fatigue Syndrome (ME/CVS), fibromyalgia or “long COVID”
*Corresponding Author : Frank Comhaire
Professor Emeritus, Department of Endocrinology
and Metabolic Diseases, Ghent University, Belgium.
Tel: +32 475 618 555;
Email: frank.comhaire@telenet.be
Received : Feb 05, 2025
Accepted : Mar 06, 2025
Published : Mar 13, 2025
Archived : www.jcimcr.org
Copyright : © Comhaire F (2025).
Abstract
Common to Myalgic encephalomyelitis, chronic fatigue syndrome and so-called long Covid is the panoply of complaints, with Post Exertional Malaise (PEM) as the most typical symptom. Added to that are permanent feeling of fatigue, decreased capacity to concentrate, so-called brain fog, non restorative sleep, diffuse pain, and – in case of long Covid – respiratory distress. Several recent studies have confirmed my original hypothesis that poor metabolism and energy production by the mitochondria are responsible for the majority of these phenomena. I have suggested that inhibition of Pyruvate dehydrogenase (Pdh) activity is the major reason for this. Pdh inhibition is probably caused by the excess of the phosphatase: Pyruvate Dehydrogenase Kinase (PDK). The latter results from “Systemic Immune Disorder” (what I called “SID”) and inflammation. Based on this hypothesis I have applied oral and infusion treatment modalities which were successful in approximately 80% of 130 consecutive patients. The pivotal substances are sodium dichloroacetate, that reduces PDK, Meldonium, that facilitates intracellular glucose metabolism, and low dose Nalexone, that optimises the function of microglia.
Keywords: ME/CFS; Myalgic encephalomyelitis; Chronic fatigue syndrome; Fatigue disease; Long-Covid; Fibromyalgia; Meldonium; Neurospect.
Citation: Comhaire F. How I treat my patients with Myalgic Encephalomyelitis, Chronic Fatigue Syndrome (ME/CVS), Fibromyalgia or “long COVID”. J Clin Images Med Case Rep. 2025; 6(3): 3508.
Introduction
In order for the body to function normally it requires energy, mainly as Adenosine Triphosphate (ATP). That is reduced to adenosine diphosphate and adenosine monophosphate in the target cells of organs. ATP is generated from glucose and from fatty acids ingested in food. This metabolic process requires several biochemical steps that are facilitated by enzymes. When glucose reaches the cells through the blood stream it must pass through the outer cell membrane. This process requires insulin, secreted by the pancreas, to bind to receptors on the cell membrane. If the secretion of insulin is decreased, glucose uptake is disturbed, and the glucose metabolism is deficient, which can result in diabetes. Alternatively, the insulin receptors may be functionally defective, and insulin binding is inadequate. This is called insulin resistance, and causes the cellular uptake of glucose to be impaired [1]. In the interior of the cells glucose, that is build up of 6 carbon atoms, must be split into two molecules containing each 3 carbon atoms, and that is called pyruvate. This process is called glycolysis. Glycolysis does not require oxygen. The “anaerobic metabolism” and the Cori cycle produce ATP, but have the inconvenience to also generate excess lactate [2].
Next, the pyruvate enters the so-called “energy centrals” of the cells, being the mitochondria. Inside the mitochondria, which are extremely small (hardly visible though the light microscope, and therefore called “sub-microscopic”) pyruvate is metabolised to efficiently generate energy. This requires the presence of oxygen and is called “aerobic metabolism”. In the first step of the process one carbon atom is remove from pyruvate, and eliminated after binding to oxygen, resulting in CO2 that is eliminated by respiration. This critical metabolic step is facilitated by the enzyme Pyruvate dehydrogenase (Pdh). The newly formed molecule (Acetyl-coenzyme A) contains only 2 carbon atoms, and is further broken down in what is called the “Krebs cycle” (also called “Citric acid cycle”). This consists of a sequence of metabolic steps facilitated by specific enzymes, generating a relatively large quantity of ATP.
The Krebs cycle also metabolises fatty acids, that need to be entered into the mitochondria thanks to the transporter protein carnitine, that is derived from amino acids. The metabolism of fatty acids also generates ATP, but it also acidifies the blood by the production of ketones, which may exert a toxic effect if present in high concentration. Fatty acid metabolism competes with pyruvate for the Krebs cycle.
Any step in this complicated sequence of metabolic processes will result in disturbed production of energy, that may cause most of the signs and symptoms of ME/CFS.
Pathogenesis
Disturbance of any of the successive steps in the metabolic process from nutritional glucose uptake to the production of energy, as well as the accumulation of lactate, cause abnormal fatigue, “post exertional malaise” (P.E.M.), functional impairment of the central nervous system, and diffuse muscular pain.
Insulin resistance diminishes the entry of glucose through the cell membrane and reducing its transfer into the cellular cytoplasm. Insulin resistance [1] commonly is part of the metabolic syndrome [3], in which case the latter diagnosis should be given, rather than ME/CFS. If insulin resistance is due to oxidative damage to the receptor as a result from general oxidative stress from inflammation, it may considered as an element of the pathogenesis of ME/CFS. Next glycolysis from glucose (with 6 carbon atoms ) to pyruvate (with 3 carbon atoms) may be deficient due a genetic defect of the enzyme system. In this case fatigue should not be attributed to ME/CFS.
The transportation of pyruvate through the outer membrane of the mitochondria takes place passively through large channels. Pyruvate then comes in contact with the enzymes of the inner membrane of the mitochondria, where oxygen causes the molecule to loose another carbon atom that is eliminated as CO2 . The resulting product, called Acetyl Co-A build of only 2 carbon atoms, is further metabolised by an sequence of reactions in what is called the Krebs cycle. This cycle is the main source of energy by efficiently generating ATP, but also some Reactive Oxygen Species (ROS). It is rather complicated sequence of metabolic changes that are facilitated by specific enzymes.
The reaction from pyruvate to Acetyl Co-A is activated by the very important enzyme Pyruvate dehydrogenase (Pdh). However the activity of Pdh can be inhibited by its opponent, the phosphatase: Pyruvate Dehydrogenase Kinase (PDK). The healthy equilibrium between Pdh and PDK can be disturbed in favour of PDK, reducing the activity of Pdh. The production of Acetyl Co-A and, subsequently, the production of energy by the Krebs cycle are reduced. Disturbance of Pdh/PDK equilibrium occurs in case of inflammation and/or immunologic disorder [4]. In ME/CFS the inhibited Pdh activity, due to excess PDK, is probably the most important mechanism causing poor energy (ATP) production by the cells, and the resulting fatigue and cerebral dysfunction. In fact, poorly efficient ATP production also impairs the pump functions (sodium-potassium pump, calcium pump) which are activated by ATP-ase in the cell membrane.
As far as fibromyalgic pain is concerned, there are additional factors that play a role, among which the enhanced connectivity between pain centres in the brain is probably the most relevant [5]. The peripheral pain stimulus is captured by specific “nociceptors” and transferred to the brain, through the spinal cord. There is evidence that this transportation may be enhanced in fibromyalgia patients [6]. The stimulus arrives at the part of the brain, called the thalamus, located at the brain base. From there, the pain message is relayed to the brain cortex, where the pain sensation is perceived. Another pathway in the brain ascertains that the pain sensation will be suppressed or dampened. The connection between the thalamus and brain cortex takes place through a bundle of neuronic “wires” called axons. The efficacy of this connecting system may be increased and its capacity to relay the pain signal may be amplified. Thus, even minor signals from the nociceptors are perceived more intensely. Also the dampening pathway may be less efficient (“disinhibition”), enhancing pain perception by the frontal brain cortex [5]. Optimal function of the cerebral neurones requires support, protection and nutrition from the microglial cells. There is strong evidence that the activity of these cells is disturbed in patients with ME/CFS due to infectious, inflammatory, immunological or metabolic causes [7]. This could result in cognitive impairment, problems with memory and concentration, as well as the so-called “brain fog”. These phenomena are enhanced by the increased concentration of lactate in the cerebrospinal fluid, due to the excessive anaerobic glucose metabolism.
Intake procedure of a new patient
The first step of intake procedure of a new patient includes in depth history taking of the personal and family precedents, as well as the symptoms at the level of different systems [8]. Patient should give details about the circumstances or events which have occurred at the start of their disease, or which caused exacerbation of signs and symptoms. A family history of disease, such as diabetes, autoimmune disease, psychiatric disorders, etc. are relevant.
Much attention should be given to the exact description and severity of the most disturbing signs and symptoms, and their influence on the professional, social, educative and personal life. I find the nine items questionnaire “Fatigue Severity Score” (FSS), [9] very useful for this purpose. Next a general propaedeutic examination should take place, with special attention to swelling of lymph nodes, “trigger points”, and any sings of autoimmune disease (such as psoriasis, Sjögren syndrome, vitiligo, alopecia, axial ankylosing spondylitis, multiple sclerosis, systemic lupus, etc.). Blood and urine analysis should include routine biological tests of all organs [10], and additional tests must assess endocrine, metabolic, inflammation and immunologic variables. Even relatively minor, and seemingly irrelevant abnormalities should be explored in detail, since they may have a major impact and must be treated appropriately.
Insulin resistance is revealed by an elevated concentration the haemoglobin A1c in blood. With that, the measurement of C-peptide and insulin in blood, taken 2 to 4 hours after a meal, is recommended [11]. Immunologic screening test include both lymphocyte cluster differentiation, as well as the measurement of Anti Nuclear Antibodies (ANA), immunoglobulins (M, A and G) and serum complement concentrations. It may be relevant to assess the specific IgM and IgG concentration against EpsteinBarr virus, herpes 6 and 7, and Borrelia. Routine Inflammatory markers are blood sedimentation rate, C-Reactive Protein (CRP) and alfa2 globulin concentrations.
Additional imaging examinations as well as e.g. neurologic test may be indicated. I find the non-invasive NeuroSpect scan highly relevant, since it typically reveals decreased blood supply to the supra optic frontal region, and to the nerve centres of the brain stem [12,13]. NeuroSpect may also detect abnormal blood supply to the limbic system suggesting emotional disfunction, or even psychiatric disease. Preferentially, it is combined with CT scan or NMR of the brain.
Treatment
Chordoma There is no treatment that fits all, since a large number of factors and pathogenic steps interfere and these are different among patients. Treating the cause of the disease is often impossible, as the initial causal event is situated in the past. These may have occurred many years before, and may have initiated the fatigue disease that has become permanent, perhaps through epigenetic or sometimes anatomical changes. In exceptional cases there may be an ongoing active infection. The latter may be the case of long-COVID, where residual (fragments of) Coronavirus are sometimes found, and also in Herpes 6/7 (Cytomegaly) infection [14], or Ebstein-Barr virus persistence. Appropriate, sometimes long-term anti-viral medication may be successful in some of these cases. Furthermore, any co-morbidity needs to be treated lege artis, in collaboration with the designated specialist.
The second best approach will attempt to correct the mechanisms by which the signs and symptoms of ME/CFS are provoked. Hereby it is mandatory to focus on metabolic dysfunction, immunologic factors, inflammation, oxidative overload, abnormal blood supply, mental impairment, and other aspects.
Oral therapy
The activity of Pyruvate dehydrogenase (Pdh) can be increased through inhibiting the Pyruvate Dehydrogenase Kinase (PDK) by means of sodium Dichloroacetate (DCA) [15]. This molecule is derived from of acetic acid, to which two chlorine atoms have been introduced. It is the natural constituent of red algae (Rhodophyseae), and is is manufactured chemically as sodiumsalt in pure form by differents laboratories . As long as the daily dose does not exceed 12.5 mg/Kg body weight, this substance is not toxic. In the food supplement that I prescribe, 400 mg of DCA is combined with 100 mg of Vitamin B1 (Thiamine), 50 mg of Alfa-lipoic acid, and 25 mg of oxidoreductase Ubiquinol Q10. These ingredients are entered into vegetarian capsules, of which patients must take one per day.
Based on the result of the Fatigue Severity Score, it is possible to predict rather accurately (AUC: 0,92) which patients will, or will not respond favourably to DCA treatment [16].
Meldonium is a pharmaceutical that has been developed by Prof Kalvins I, Latvia (1970) and manufactured by the Grindeks company as Mildronate®. Meldonium inhibits the bio-synthesis of l-carnitine [17]. By reducing I-carnitine the fatty acid transportation into the cellular mitochondria is diminished. Glucose-pyruvate metabolism via the Kreb’s cycle thus takes predominance in the competition with fatty acids, resulting in the increased production of Adenosine Triphosphate (ATP), so more energy. Because the aerobic glucose production is facilitated, the anaerobic metabolism (and through the Cori cycle) diminishes, and so does the production of lactate during exercise and brain activity.
More recently Low Dose Naltrexone (LDN), of only 4,5 mg per day, has been introduced for the treatment of patients suffering from fibromyalgia and CFS [18]. Its mechanism of action is only partly elucidated, and seems to be by improving (micro) glial cell function. Glial cells provide physical and chemical support to neurons and maintain their optimal environment. They exert a nutritional function, suppress infection, and sustain immunologic resistance. Patients taking Naltrexone LDN enjoy greater wellbeing, less fatigue, improved mood, and less pain.
QALY® (Jonapharma, Elversele, Belgium) is a nutraceutical containing minerals, plant extracts, vitamins, the biomass of Haematococcus pluvialis, and oil of arctic krill [19,20]. These exert antioxidant, anti inflammatory and adaptogenic activities, making this composite natural food supplement particularly suitable for ME/CFS patients. Its main components are described below.
The natural extract of the Mediterranean pine tree is rich in anthocyanidins that exert a strong anti-inflammatory as well as anti-oxidant activity. It also reduces auto-immune reactivity. Its therapeutic and protective potentials have been objectively documented [21]. It reduces muscular and articular pain, decrease the blood concentration of mediators of inflammation (such as CRP), and increases the redox capacity.
The extract of Rhodiola rosea extract belongs to the group of substances called an “adaptogens” [22]. These agents interact with the biological stress response by mitigating the hypothalamo-pituitary-adrenal (HPA) reaction, and by augmenting the concentration of Heat Shock Protein (HSP) that reduces the effects of stress on protein folding. This phytotherapeutical adaptogen reduces the deleterious effects of all levels of stress on both mental and the physical health.
QALY® also contains the readily absorbable form of two essential minerals, namely the bisglycinate of zinc and seleniomethionine.
When taken together with vitamin B6, Zinc (bisglycinate) plays an important role in the conversion of the essential omega-3 short-chain fatty acids, such as alpha linolenic acid, into long-chain polyunsaturated fatty acids (PUFA), in particular eicosapentaenoic acid (EPA) and docosahexaenoic acid or cervonic acid (DHA). Zinc and vitamin B6 are necessary for the elongase and desaturase processes that are needed in this conversion The anti-inflammatory properties of these PUFA’s have been demonstrated [23], amongst others in patients with rheumatoid arthritis and similar conditions. Zinc is also recommended for DNA stability, protecting against mutations, and it is an essential mineral in many enzymatic processes required for cellular metabolism.
Selenomethionine has a strong antioxidant effect, protecting against oxidative damage to DNA. It is a co-factor of glutathione peroxidase, that is the most potent detoxifying agent in the human body. When given in combination with the oxidoreductase ubiquinol Q10, Selenomethionine reduces cardiovascular mortality by 40%. Selenomethionine has been proven to boost the immune response and to reduce inflammation in response to viral infections. Since suboptimal selenium concentration in blood is associated with mental dysfunction that is commonly found in ME/CFS patients, supplementation is recommended [24].
Oxidative overload results from inflammation or infectious conditions. Reactive oxygen species are also produced during the Cori- and the Krebs cycles of the anaerobic and the aerobic metabolism of glucose, lactate and fatty acids. Oxidative stress has deleterious effects on all organ functions by converting the fatty acid composition of the cellular membrane from Poly Unsaturated Acids (PUFA) to saturated acids, reducing membrane fluidity, the three dimensional structure of receptors, and pump functions. Several antioxidants address different aspects of oxidative stress.
Astaxanthin is a carotenoid that does not display the toxic and teratogenic side effects of (high-dose) Vitamin A. It is strong antioxidant which is abundantly present in the biomass of the microscopic Haematococcus pluvialis. Astaxanthin has multiple beneficial effects by stabilizing the fatty acid composition of cell membrane. It prevents the nucleotides (in particular Guanine) of DNA from being converted to their oxidized form (e.g. 8hydroxy-2-deoxyguanosine), which displays teratogenic potential. Astaxanthin supplementation was found to ameliorate fatigue and mental function in ME/CFS patients [25].
The oxidoreductase ubiquinone Q10 plays an important role in maintaining optimal mitochondrial function and energy production of Adenosine Triphosphate (ATP). Q10 absorbs reactive oxygen species produced during glucose metabolism [24]. It promotes muscle function, and is necessary for the proper contraction of the heart.
The combination of vitamins B9 with B12 reduces the concentration of homocysteine in the blood. A elevated homocysteine level accelerates brain shrinkage, which has been observed is patients with ME/CFS. These vitamins can help to prevent the memory loss and deficient cognitive function that are often occurring after viral infection, such as typically recorded in “long Covid” patients. In patients with ME/CFS and fibromyalgia the food supplementation with these vitamins was found to significantly reduce pain [26].
Infusion therapy
Infusion therapy is proposed during the initial phase of treatment of ME/CFS patients. Thereby intravenous infusion of physiological salt solution is administered slowly over a time span of one to two hours. I use an adaptation of “Meyers’” cocktail [27,28]. The infusion fluid contains Magnesium sulphate, usually in a dose of 2 grams, together with a complete panoply of vitamins (such as in Cernevit®, Baxter SA, Lessines, Belgium), and glutathione. These infusions are given every fortnight, often together with oral treatment. Intervals between infusions are extended when patients start to feel better. It can be intensified as soon as fatigue becomes more prominent again, such as after a (viral) infection or a period of stress.
Outcome of therapy
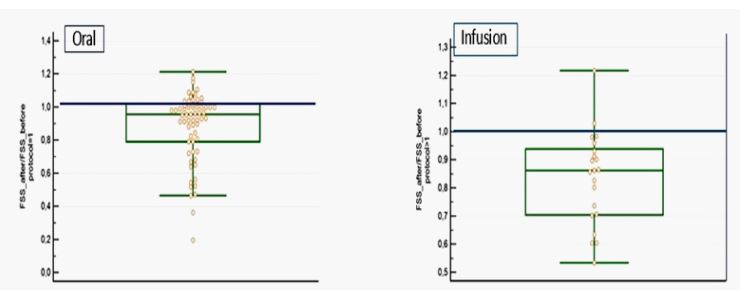
Based on experience and follow-up of approximately 150 patients, of which 130 subsequent cases were statistically analysed with the Fatigue Severity Score (FSS) questionnaire, more than 80% reported improvement of their condition. In the NeuroSpect investigation, a significant enhancement of blood supply was objectivated in both the prefrontal supraorbital region, and in the nerve centres of the brain stem [29]. Based on the subclasses of the FSS questionnaire, it was possible to predict rather accurately which patients will, or will not favourably respond to the oral therapy.
The degree of improvement was, however, remarkably different among patients, varying from moderate to impressive (Figure 1) [30]. The response was independent from the pretreatment status. It can be seen that the degree of improvement was similar in the group of patients treated by oral therapy, as compared to those treated by infusions. However, a larger proportion of patients continued oral therapy.
Therapeutic results were maintained during follow-up of many months to years, and most patients could resume their familial and/or professional activities, albeit usually only on a part-time basis.
None of the patients reported significant side effects. Vital variables and biology remained unaffected, except for the immunological parameter Anti-Nuclear-Antibodies (ANA), the titre of which decreased in some of them.
Acknowledgements: The author expresses his gratitude to Jan Pen MD. PhD who participated in the prospective clinical trials. He thanks DCA lab (Curaltus Ltd, Vilnius, Lithuania) for providing the sodium dichloroacetate formulation.
References
- Freeman AM, Acevedo LA, Pennings N. Insulin Resistance. NCBI Bookshelf. National Library of Medicine, NIH. Updated August 17, 2023.
- Monireh Dashty. A quick look at biochemistry: carbohydrate metabolism. Clinical Biochemistry. 2023; 46(15): 1339-1352. doi. org/10.1016/j.clinbiochem.2013.04.027.
- Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech. 2009; 2(5-6): 231-237. doi:10.1242/ dmm.001180.
- Stacpoole PW. Therapeutic targeting of the pyruvate dehydrogenase Complex/ pyruvate dehydrogenase kinase (PCC/PDK) axis in cancer. JNCI 2017, djx071. doi.org/10.1093/jnci/djx071.
- De Ridder D, Vanneste S, Smith M, Adhia D. Pain and the triple network model. Front Neurol. 2022; 13: 757241.doi:10.3389/ fneur.2022.757241.
- Marshall A, Burgess J, Goebel A, Bernhard F, et al. Evidence for spinal disinhibition as a pain-generating mechanism in fibromyalgia syndrome. Pain Reports. 2025; 10(1): pe1236. doi: 10.1097/PR9.
- Nakatomi Y, Mizuno K, Ishii A, Wada Y, et al. Neuroinflammation in patients with Chronic Fatigue syndrome/Myalgic Encephalomyelitis: An11C-®-PK11195 PET study. JNM. 2014; 55 (6): 945- 950. doi.org/10.2967/jnumed.113.131045.
- NICE guidelines (NG206). Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. Published 29 October 2021.
- Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. http://www.mult-scjerosis. org/fatigueseverityscale.html. 1989. Arch Neurol. 1989; 45(10): 1121-1123. doi: 10.1001/archneur.1989.00520460115022;
- CDC. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Evaluation of ME/CFS, May10, 2024.
- Khan HA, Sobki SH, Ekhzaimy A, Khan I, Almusawi M. Biomarker potential of C-peptide for screening of insulin resistance in diabetic and non-diabetic individuals. Saudi J Biol Sci. 2018; 25(8): 1729-1732. doi: 10.1016/j.sjbs.2018.05.027.
- Costa DC, Tannock C, Brostoff J. Brainstem perfusion is impaired in chronic fatigue syndrome. QJM. 1995; 88(11): 767-773.
- Fischler B, D’Haenens H, Cluydts R, Michiels V et al. Comparison of 99Tc HMPAO SPECT scan between chronic fatigues syndrome, major depression and healthy controls: an exploratory study of clinical correlates of regional cerebral blood flow. Neuropsychobiology. 1996; 34(4): 175-183.
- Pantry SN, Medveczky MM, Arbucle JH, Luka J, et al. Persistent human herpesvirus-6 infection in patients with an inherited form of the virus. Journal of Medical Virology. 2013; 25: 2013. doi.org/10.1002/jmv 23685.
- Comhaire F. Treating patients suffering from Myalgic Encephalopathy/Chronic Fatigue Syndrome (ME/CFS) with sodium dichloroacetate: an open-label, proof-of-principle pilot trial. Medical Hypothesis. 2018; 114: 45-48. doi: 10.1016/mehy.2018.03.002.
- Comhaire F. Why do some ME/CFS patients benefit from treatment with sodium dichloroacetate, but others do not? Medical Hypotheses. 2018; 120: 65-67. doi: 10.1016/j.mehy.2018.08.014
- Dombrova M, Makrecka-Kuka M, Vilskersts R, Mackrarova E, et al. Pharmacological effects of Meldonium: biochemical mechanisms and biomarkers of cardiometabolic activity. Pharmacological Research. 2016; 113(B): 771-780. doi10.1015/j. phrs.2016.01.019.
- Yang J, Shin K-M, Do A, Bierle DM. et al. The safety and efficacy of Low-Dose Naltrexone in patients with fibromyalgia: A Systematic Review. J Pain Res. 2023; 16: 1017–1023. doi: 10.2147/JPR. S395457.eCollection 2023.
- Comhaire F, Decleer W. Can the biological mechanisms of ageing be corrected by food supplementation. The concept of health care over sick care. Aging Male 2020; 23(5): 1146-1157. doi: 10.1080/13685538.2020.1713080.
- Comhaire F, Decleer W, Deslypere JP. Adding Quality Adjusted Life-Years (QALY’s) by nutraceutical food supplementation. JCRMHS 2023; 5(1): 1-6.
- Weichmann F, Rohdewald P. Pycnogenol® French maritime pine bark extract in randomized, double-blind, placebo-controlled human clinical studies. Front Nutr. 2024; 11: 1389374. doi: 10.3389/fnut.2024.1389374.
- Machin RP, Florido M, Chirino-Godoy R, Lopez-Rios L. Adaptogenic botanicals with emphasis on Rhodiola rosea and Withania somnifera. Eur J Medicinal Plants. 2023; 34 (11): 20-39.
- Oppedisano F, Macri R, Gliozzi M, Musolino V, et al. The anti-inflammatory and antioxidant properties of N-3 PUFAs: their role in cardiovascular protection. Biomedicines. 2020; 8(9): 306. doi: 10.10.3390/biomedicines8090306..
- Castro-Marrero J, Domingo JC, Cordobilla B, Ferrer R, et al. Does coenzyme Q10 plus selenium supplement ameliorate clinical outcomes by modulating oxidative stress and inflammation in individuals with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome? Antioxid Redox Signal. 2022; 36(10): 729-739. doi:10.1089/ats.2022.0018.
- Imai A, Oda Y, Ito N, Seki S, et al. Effects of dietary supplementation of Astaxanthin and Sesamin on daily fatigue: a randomize, double-blind, placebo-controlled, two-way crossover study. Nutrients. 2018; 10(3): 281. doi: 10.3390/nu10030281.
- Regland B, Forsmark S, Halaouate L, Matousek M, et al. Response to Vitamin B12 and Folic acid in Myalgic Encephalomyelitis and Fibromyalgia. PloS One. 2015; 10(4): e0124648. doi: 10.1371/journal.pone.0124648.
- Gaby AR. Intravenous nutrient therapy: the “Meyers’ cocktail”. Altern Med Rev. 2002; 7(5): 389-403.
- Ali A, Njike VY, Northrup V, Sabina AB, et al. Intravenous micronutrient therapy (Meyers’ cocktail) for fibromyalgia: a placebocontrolled pilot study. J Altern Complement Med. 2009; 15(3): 247-257. doi: 10.1089/acm.2008.0410.
- Comhaire F, Deslypere JP. News and views in myalgic encephalomyelitis /chronic fatigue syndrome (ME/CFS): the role of comorbidity and novel treatments. Med Hypotheses 2020; 134: 109444. doi: 10.1016.mehy.2019.109444.
- Pen J, Comhaire F. Treating Post-Covid & Chronic Fatigue Syndrome (ME/CFS). Acta Clinica Belgica. 2019. Society of Internal Medicine. 13-14 dec. La Hulpe, Belgium.