Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Severe complications of mechanical ventilation: Subcutaneous and mediastinal emphysema
*Corresponding Author : Xueqi Li
Associate Professor, Institute of Computing
Technology, Chinese Academy of Sciences (ICT,
CAS), China.
Email: zwxzdsj@163.com
Received : Feb 05, 2025
Accepted : Mar 07, 2025
Published : Mar 14, 2025
Archived : www.jcimcr.org
Copyright : © Xueqi L (2025).
Citation: Xueqi L. Severe complications of mechanical ventilation: Subcutaneous and mediastinal emphysema. J Clin Images Med Case Rep. 2025; 6(3): 3510.
Description
A 62-year-old man with a history of Chronic Obstructive Pulmonary Disease (COPD) presented to the emergency department with an eight-hour history of dyspnea and vomiting coffee-colored substance following heavy alcohol consumption (200 ml Baijiu and 2500 ml beer). Despite being in a stupor state, his oxygen saturation was alarmingly low at 81%, and he exhibited tachypnea (40 breaths per minute). Physical examination revealed generalized wheezing. Blood gas analysis showed a pH of 7.20, PO2 of 59 mmHg, and lactate level of 12.11 mmol/L.
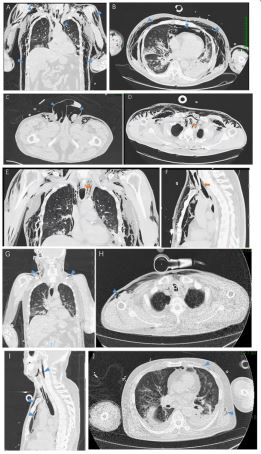
The patient’s condition deteriorated rapidly, necessitating urgent tracheal intubation to protect his airway and improve ventilation. Mechanical ventilation led to gradual improvement in oxygenation. However, twelve hours later, the patient developed severe scrotal swelling, and extensive crepitus was palpable over the neck, chest, abdomen, and both upper limbs. Computed Tomography (CT) scan revealed extensive subcutaneous emphysema (Figure 1A-1C, arrowheads), along with a tracheal perforation at the T1 segment (Figure 1D-1E, arrows), accompanied by mediastinal emphysema.
To address the tracheal perforation, we deepened the endotracheal tube by 2 cm to isolate the site of injury using a balloon. Ventilator parameters were adjusted to minimize gas entry into the subcutaneous and mediastinal spaces. Meticulous observation ensured that the emphysema did not worsen. Follow-up imaging 36 hours later demonstrated significant reduction in emphysema (Figure 1G-1J, arrowheads). Active treatment led to overall improvement, and the patient’s tracheal intubation was subsequently removed.
This case highlights the importance of vigilance during tracheal intubation. The guide wire’s length should never extend beyond the endotracheal tube to prevent stretching and potential complications. Adjusting the depth of endotracheal intubation can effectively manage subcutaneous and mediastinal emphysema. Clinicians should be aware of this rare but critical complication and consider timely interventions such as tracheotomy or subcutaneous incisions if emphysema persists.