
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Salicylate-induced heart block: A silent alarm
Nidha Shapoo*; Natoushka Trenard; Armeen Poor
Department of Pulmonary and Critical Care, New York Medical College/Metropolitan Hospital, New York, USA.
*Corresponding Author : Nidha Shapoo
Department of Pulmonary and Critical Care, New
York Medical College/Metropolitan Hospital, New
York, USA.
Email: shapoon@nychhc.org
Received : Feb 07, 2025
Accepted : Mar 10, 2025
Published : Mar 17, 2025
Archived : www.jcimcr.org
Copyright : © Shapoo N (2025).
Abstract
Salicylate toxicity can involve multiple organ systems, particularly the central nervous system, the pulmonary system, and the gastrointestinal system. Cardiac dysrhythmias and heart blocks are rarely seen with salicylate toxicity. We present here a 67-year-old male who was brought to the emergency department with an altered mental state. The patient had a known history of schizophrenia and polysubstance abuse. Venous blood gas was suggestive of mixed respiratory alkalosis and metabolic acidosis. Serum salicylate level was 67.1 mg/dl. After initial fluid resuscitation and sodium bicarbonate therapy, urgent hemodialysis was initiated. During the hospitalization, the patient developed bradycardia followed by second-degree heart block. The patient was kept on telemetry with regular monitoring of serum electrolytes. The electrophysiological studies of the heart did not show any abnormality. The patient recovered spontaneously. Serum salicylate returned to the sub-therapeutic levels. The patient was discharged in a stable condition. This case highlights a serious complication of salicylate toxicity, which demands early attention to avoid morbidity and mortality.
Citation: Shapoo N, Trenard N, Poor A. Salicylate-induced heart block: A silent alarm. J Clin Images Med Case Rep. 2025; 6(3): 3512.
Introduction
Salicylates are found in over-the-counter medications, including aspirin, bismuth subsalicylate, effervescent antacids, ointments, liniments, and oil of wintergreen (methyl salicylate), and alternative medication products (e.g., willow bark) [1]. Acute salicylate toxicity generally occurs in young adults with a history of psychiatric illness who tend to overdose in a suicide attempt. The onset of symptoms occurs within 3 to 8 hours, and the severity depends on the amount ingested. The clinical manifestations generally occur when the plasma levels exceed 40 or 50 mg per deciliter and include tinnitus, vertigo, nausea, vomiting, and hyperpnea. Severe intoxication occurs between 50 mg per deciliter and 70 mg per deciliter and can be associated with fever, sweating listlessness, and incoordination. At levels exceeding 75 mg per deciliter, patients are at risk for hallucinations, seizures, cerebral edema, coma, noncardiogenic pulmonary edema, and cardiovascular collapse [2,3]. Cardiac dysrhythmias and heart blocks are extremely rare with salicylate toxicity, and only three cases have been reported so far [4,6].
We, here, report a patient who was admitted with acute salicylate toxicity and developed second degree heart block during the hospitalization. This is the second case of heart block associated with salicylate toxicity. The first case was reported with chronic salicylate toxicity [4].
Case presentation
A 67-year-old male with a past medical history of schizophrenia, asthma, and polysubstance use disorder was brought to the Emergency Department (ED) because of an altered mental state. Upon arrival at ED, the patient was drowsy, arousable to minor stimuli, and noted to have right-sided facial droop. There was no focal weakness and no history of seizures. The history of drug toxicity was not clear. As per the clinical supervisor of his shelter, the patient had a history of drinking large amounts of Nyquil (acetaminophen 650 mg/dextromethorphan 30 mg/ doxylamine succinate 12.5 mg. Patient was afebrile, HR-92, RR16, BP-118/77 mmHg, SPO2 -98% on room air. The patient was evaluated by the stroke team at the bedside and put on the monitor, and stroke protocol was followed. The Poison Control team was consulted, and the patient was evaluated for substance abuse. Labs revealed; hemoglobin: 12.3 g/dl, WBC 3.58 x103 /mcL, blood sugar 106 mg/dl, creatinine 1.1 mg/dl, sodium 140 mEq/L, potassium-3.4 mEq/L, bicarbonate-15 mmol/L, magnesium-2.3 mg/dl, urine toxicology was negative, PT/INR29/2.5, serum ethanol, lithium and acetaminophen levels were negative. The computed tomography head showed an early left middle cerebral artery infarct. The patient was loaded with clopidogrel 300 mg and lipitor 80 mg. Neurology was consulted for possible left MCA thrombectomy, but the patient was deemed not a candidate for thrombectomy and tPA as the window for the stroke was unknown. The patient was put on close monitoring and frequent neurochecks for signs of neurologic deterioration. Serum salicylate level came as 67.1 mg/dl. Venous blood gas showed Ph-7.47, Pco2 -25, PO2 -31, lactate-1.1, and bicarbonate-20, suggestive of mixed respiratory alkalosis and metabolic acidosis. Initial Electrocardiogram (ECG) showed normal sinus rhythm and right bundle branch block, similar to previous ECGs. The patient was given a bolus of 1 meq of bicarbonate and started on bicarbonate infusion to maintain urine pH >7. The patient was admitted to the ICU and put on telemetry. Nephrology was consulted for urgent hemodialysis because of an altered sensorium. The patient underwent 3 hours of hemodialysis, and the serum salicylate level dropped to 25 mg/dl post-hemodialysis. Venous blood gas showed pH-7.4, pO2 -42, pCO2 -28, and bicarbonate-28. The patient’s mental status improved, but he continued to be lethargic.
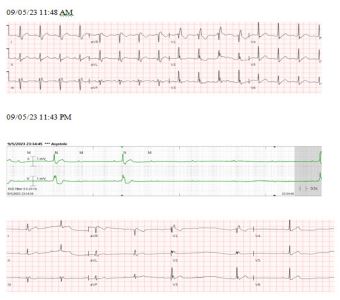
On the same day of admission at 11:30 pm, the patient became agitated with a heart rate of 40/min, blood pressure of 70/50 mmHg, and went into asystole for a few seconds. The patient was given atropine push and dextrose 25 gm, and the patient recovered within 3 seconds. ECG showed sinus bradycardia with a 2nd-degree A-V block (Mobitz II) and a right bundle branch block. Telemetry showed evidence of second-degree type 2 AV block, with dropped beats and pauses lasting longer than >6 seconds. Serum electrolytes and blood sugar were normal.
Cardiology was consulted, and the patient was planned for electrophysiological studies and possible pacemaker insertion.
On the second day of admission, the patient became conscious and oriented. On questioning, the patient admitted that he took half a bottle of unknown medication to kill bugs in his stomach. Psychiatry was consulted. Antipsychotics could not be prescribed because of bradycardia and AV block. An echocardiogram was done, which showed normal left ventricular systolic and diastolic function with a left ventricular ejection fraction of 55%-60%. Telemetry was reviewed, which showed bradycardia with the occasionally dropped beat. However, the frequency was significantly less compared to the previous day.
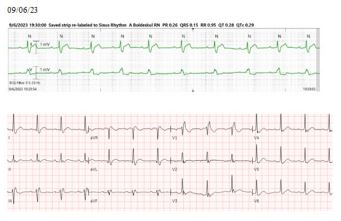
The patient remained on telemetry, regularly monitoring electrolytes and salicylate levels. Electrophysiological studies did not reveal any abnormality. The patient recovered spontaneously without any further evidence of dropped beats or AV block. CT angiography of the brain was done for the concerns of left MCA infarct, which did not reveal any intracranial or cervical artery occlusion or stenosis. The patient was discharged from the ICU and transferred to the psychiatry unit for the management of schizophrenia and psychosis. After stabilization, the patient was discharged safely.
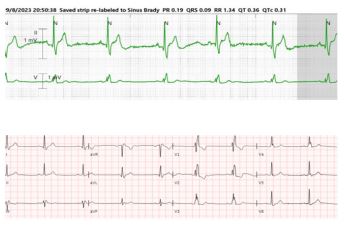
Table 1: Serial salicylate levels.
| 09/05/23 11:30 AM | 09/05/23 04:17 PM | 09/05/23 10:00 PM | 09/06/23 01:46 AM | 09/06/23 11:06 AM | 09/09/23 06:26 AM | |
|---|---|---|---|---|---|---|
| Salicylate level (mg/dl) | 67.1 | 58.7 | 25.3 | 24.5 | 16 | < 1 |
Discussion
Salicylate toxicity affects multiple cellular and systemic mechanisms, but the principal pathophysiologic mechanism is interference with aerobic metabolism utilizing uncoupling of mitochondrial oxidative phosphorylation leading to metabolic acidosis. Toxic levels activate the respiratory center of the medulla, causing tachypnea, hyperventilation, respiratory alkalosis, increased renal elimination of HCO3 , and increased insensible fluid loss [3]. Salicylate-induced acid-base changes begin with respiratory alkalosis, followed by mixed respiratory alkalosis-metabolic acidosis, and finally, metabolic acidosis [7].
Classical salicylism presents as a triad of hyperventilation, tinnitus, and Gastrointestinal (GI) irritation. Patients who present early in the course of salicylate toxicity may have modest symptoms, but patients who present late may manifest altered mental status (e.g., agitation, confusion, restlessness, seizures, coma), noncardiac pulmonary edema, cerebral edema, and death [2,3,8-11]. Our patient presented with altered mental status, which was initially confused with a stroke.
There is no specific antidote for salicylate toxicity. The treatment includes fluid resuscitation and serum alkalization to increase the elimination of salicylate and correct metabolic acidosis [12]. Electrolyte abnormalities, if any, should be corrected. Hemodialysis should be considered early in patients who have serum salicylate concentration >7.2 mmol/L (100 mg/dL) or patients who have altered mental state, refractory acidaemia, electrolyte imbalance, hyperthermia (temperature >39°C despite active cooling measures) or renal failure [13,14]. In our patient, the early initiation of hemodialysis resulted in improved recovery.
Cardiac conduction abnormalities are extremely rare in salicylate toxicity and have been reported only as case reports [4-6]. These complications can occur because of electrolyte abnormalities and/or a direct effect of salicylate on myocardial membrane permeability. In the first report of heart block [4], a 77-year-old woman was admitted with altered sensorium and difficulty breathing and was found to have chronic salicylate intoxication. She went into complete heart block and asystole, was intubated, resuscitated, and a temporary transvenous pacemaker was placed. She improved and was discharged without any cardiac deficits. In the other two reports [5,6], cardiac dysrhythmias were associated with salicylate intoxication. The arhythmias ranged from atrioventricular nodal conduction disturbances, atrial arrhythmias to monomorphic ventricular tachycardia and Torsades de Pointes. Both the patients improved after treatment and were discharged in a stable condition. Our patient developed transient heart block and asystole during the hospitalization which recovered spontaneously. The electrophysiological studies of our patient were normal, and he did not require a pacemaker.
Conclusion
Salicylate toxicity can result in heart blocks. It is important that the clinicians are aware of these potential complications. The timely institution of proper treatment can reduce the morbidity and mortality associated with salicylate toxicity.
Conflicts of interest: None
References
- American College of Medical Toxicology. Guidance document: management priorities in salicylate toxicity. J Med Toxicol. 2015; 11(1): 149-52.
- Dargan PI, Wallace CI, Jones AL. An evidence based flowchart to guide the management of acute salicylate (aspirin) overdose. Emerg Med J 2002; 19: 206-209.
- Biff F. Palmer, and Deborah J. Clegg. Salicylate Toxicity. N Engl J Med. 2020; 382: 2544-2555.
- Aggarwal N, Kupfer Y, Chawla K, Tessler S. Altered mental status and complete heart block: an unusual presentation of aspirin toxicity. BMJ Case Rep. 2013; 2013: bcr2013010083.
- Kent K, Ganetsky M, Cohen J, et al. Non-fatal ventricular dysrhythmias associated with severe salicylate toxicity. Clin Toxicol (Phila). 2008; 2013: 297–9.
- Mukerji V, Alpert MA, Flaker GC, et al. Cardiac conduction abnormalities and atrial arrhythmias associated with salicylate toxicity. Pharmacotherapy 1986; 2013: 41–3.
- Gabow PA, Anderson RJ, Potts DE, Schrier RW. Acid-base disturbances in the salicylate-intoxicated adult. Arch Intern Med 1978; 138: 1481-1484.
- Cazals Y. Auditory sensori-neural alterations induced by salicylate. Prog Neurobiol. 2000; 62:583.
- Thongprayoon C, Lapumnuaypol K, Kaewput W, et al. Gastrointestinal bleeding among hospitalizations for salicylate poisoning in the United States. QJM. 2021; 114:190.
- Rauschka H, Aboul-Enein F, Bauer J, et al. Acute cerebral white matter damage in lethal salicylate intoxication. Neurotoxicology. 2007; 28:33.
- Niehoff JM, Baltatzis PA. Adult respiratory distress syndrome induced by salicylate toxicity. Postgrad Med. 1985; 78:117.
- Proudfoot AT, Krenzelok EP, Vale JA. Position paper on urinary alkalinization. J Toxicol Clin Toxicol. 2004; 42: 1.
- Minns AB, Cantrell FL, Clark RF. Death due to acute salicylate intoxication despite dialysis. J Emerg Med. 2011; 40(5): 515-7.
- Lund B, Seifert SA, Mayersohn M. Efficacy of sustained low-efficiency dialysis in the treatment of salicylate toxicity. Nephrol Dial Transplant. 2005; 20(7): 1483-4.