
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Upper gastrointestinal bleeding secondary to Cameron lesion in three Nigerians: A case series of an under-recognized condition
Kenechukwu Okonkwo1; Oluseyi Adejumo1; Olumuyiwa Bojuwoye2; Aminu Aliyu2; Olufikemi Fabusuyi1
1Department of Internal Medicine, University of Medical Sciences, Ondo State, Nigeria.
2Department of Internal Medicine, University of Ilorin Teaching Hospital, Ilorin, Nigeria.
*Corresponding Author : Kenechukwu Okonkwo
Department of Internal Medicine, University of
Medical Sciences, Ondo State, Nigeria.
Email: circumzized@yahoo.com
Received : Feb 12, 2025
Accepted : Mar 11, 2025
Published : Mar 18, 2025
Archived : www.jcimcr.org
Copyright : © Okonkwo K (2025).
Abstract
Cameron lesion is an under-recognized cause of bleeding from the upper gastrointestinal tract especially in sub-Saharan Africa. Ulcers and/or erosions are the culprits which are seen around hiatal hernias in patients with upper gastrointestinal haemorrhage. It may be difficult to diagnose unless meticulous examination of the gastric folds is done. Most patients can usually be managed effectively with PPIs with good outcomes.
Keywords: Cameron lesion; Gastrointestinal Bleeding; Hiatal hernia.
Citation: Okonkwo K, Adejumo O, Bojuwoye O, Aliyu A, Fabusuyi O. Upper gastrointestinal bleeding secondary to Cameron lesion in three Nigerians: A case series of an under-recognized condition. J Clin Images Med Case Rep. 2025; 6(3): 3513.
Introduction
Gastrointestinal bleeding is one of the common presentations in the hospital especially in the emergency setting [1]. The common causes of upper gastrointestinal bleeding include peptic ulcer disease, erosions and ruptured oesophageal varices [1].
Cameron lesion, though implicated in the aetiology of upper gastrointestinal bleeding, has not been well described in subSaharan Africa [2]. Spontaneous healing of the lesions resulting in missed lesions could be one of the reasons why this is so especially as average time to endoscopy in the event of upper gastrointestinal bleeding in Sub-Saharan Africa is prolonged [2,3]. We present 3 cases of Cameron lesion in the setting of upper gastrointestinal haemorrhage.
Patients and observation
Case 1
Patient information: A 52-year-old female presented to the endoscopy suite with a history of recurrent vomiting for three months. Vomiting started insidiously but gradually worsened. Vomitus contained recently ingested food material. Vomiting usually occurred when patient bent forward or lifted heavy loads. After some weeks, she started vomiting blood which was usually noticed after vomiting large amounts of food. The blood sometimes was bright red and occasionally coffee ground in appearance. Blood loss was about 50 ml per episode. There was associated melaena. There was also a history of upper abdominal pain radiating to the back. There was no history of haematochezia, jaundice, body swelling, dizziness, differential limb weakness or loss of consciousness.
She is a known patient with schizophrenia who has been on Olanzapine and Amitriptyline in the last three years with good clinical response. There was no history of peptic ulcer disease, systemic hypertension or diabetes mellitus. She neither smoked cigarettes nor took alcoholic beverages. There was no prior history of blood transfusions and surgeries.
Clinical result: On examination, she was conscious and alert, pale, anicteric, acyanosed, not dehydrated, no pedal edema. Her vital signs were stable. There was epigastric abdominal tenderness. No organomegaly was detected. Ascites was not demonstrable. Bowel sounds were present and normoactive.
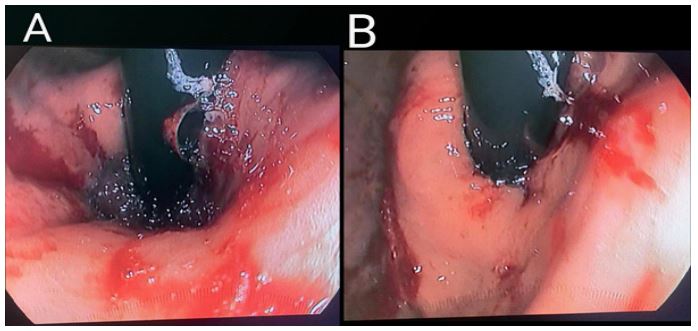
Diagnostic approach: Upper gastrointestinal endoscopy was done which revealed hiatal hernia as well as erosions with stigmata of recent bleed (Figure 1).
Therapeutic intervention and follow up: She was commenced on long term, twice daily proton pump inhibitors (PPIs) regimen with resolution of gastrointestinal bleeding. She has been seen on follow-up in the clinic twice and she is clinically stable.
Case 2
Patient information: A 45-year-old female presented to the endoscopy suite with a history of recurrent heartburn and upper abdominal pain of 6 months. Abdominal pain progressively worsened despite being on anti-ulcer agents and was worse on ingestion of spicy foods and pepper. There was a preceding history of melaena that lasted for a week. There was no history of haematochezia, jaundice, body swelling, dizziness, differential limb weakness or loss of consciousness.
There was no history of systemic hypertension or diabetes mellitus. She neither smoked cigarettes nor took alcoholic beverages. There was no prior history of blood transfusions and surgeries.
Clinical result: On examination, she was conscious and alert, pale, anicteric, acyanosed, not dehydrated, no pedal edema. Her vital signs were stable. Systemic examination was normal
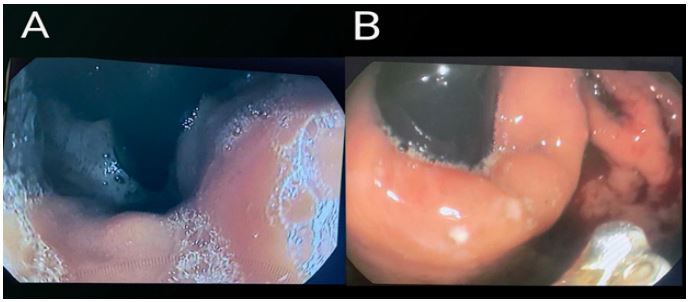
Diagnostic approach: Upper gastrointestinal endoscopy was done which revealed hiatal hernia as well as healed ulcers which were suggestive of Cameron lesions (Figure 2).
Therapeutic intervention and follow up: She was also commenced on twice daily PPIs with good clinical outcome.
Case 3
Patient information: A 53-year-old male presented to the endoscopy suite with a history of recurrent melaena of two years duration. It was sporadic, resolving on its own. There was no noticed exacerbating or relieving condition.
There was a positive history of use of herbal remedies on each episode of melaena without any improvement of clinical symptoms. He was referred for endoscopy on evaluation by a family physician.
Clinical result: On examination, he was conscious and alert, pale, anicteric, acyanosed, not dehydrated, no pedal edema. His vital signs were stable. Systemic examination was normal.
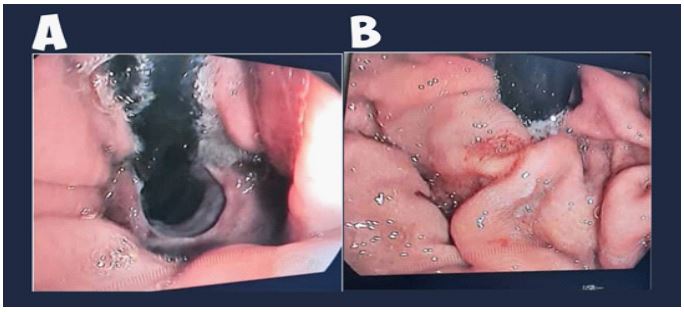
Diagnostic approach: Upper gastrointestinal endoscopy was done which revealed hiatal hernia as well as erosions which were suggestive of Cameron lesions (Figure 3).
Therapeutic intervention and follow up: He was also commenced on twice daily PPIs with good clinical outcome.
Patient perspective: The patients acknowledged that they were initially distressed by the symptoms of upper gastrointestinal bleeding. They subsequently felt better after diagnosis on endoscopy, counselling about diagnosis and treatment with PPIs.
Discussion
Cameron lesions describe single or multiple gastric erosions and/or ulcerations typically seen at the level of the diaphragmatic hiatus on upper endoscopic examination [4]. They were first documented by Cameron and Higgins in 1986 [5]. They are an established cause of upper gastrointestinal haemorrhage accounting for 0.2% of overt bleeding [6]. They occur more frequently in iron deficiency anaemia and obscure gut bleeding (1.9-9.2%) [4,7]. Cameron lesions have traditionally been thought to be the result of the mucosal sequela of mechanical trauma from hiatal hernia. It is hypothesized that as the proximal stomach is compressed, the hernia moves against the diaphragm leading to ischaemia [8]. Histopathology has also corroborated the fact that ischaemia is central to the pathophysiology of Cameron lesion [9]. Some studies have suggested that binge drinking, inadequate fiber intake and high sitting position during defecation were associated with Cameron lesions [10,11].
They are grossly underreported all over the world especially in sub-Saharan Africa as they can be missed if not thoroughly sought for [2,10]. There are only a few reports of Cameron lesions in sub-Saharan Africa [12,13]. A recent systematic review found out that at least two endoscopies had to be undertaken on the average before Cameron lesions were identified [2]. Factors that may assist in the diagnosis include meticulous observation of all gastric folds particularly around the diaphragmatic os as well as use of advanced endoscopic techniques such as narrow band imaging and chromoendoscopy [14]. They are usually seen in the mucosa of the fundus and/or corpus in association with hiatal hernias especially when the hernial sacs are larger than 5 cm [4]. This association with hiatal hernias can be helpful in the elucidation of Cameron lesion as the cause of bleeding or dyspepsia in patients on evaluation, so that repeated and unnecessary diagnostic procedures can be excluded [10]. This is the first report of Cameron lesion from Nigeria in the literature to the best of our knowledge.
We report three cases of Cameron lesions causing upper gastrointestinal haemorrhage. Two of them were females which is in keeping with the preponderance of females as previously described [2]. In the first patient, there was evidence of recent bleed i.e. oozing blood which made diagnosis relatively easy. The second patient’s diagnosis was not as easy as the healed ulcer was only perceptible after meticulous evaluation. The patient had the procedure three weeks after bleeding had subsided. In a report from Ethiopia, diagnosis was only made intraoperatively following a history of easy fatiguability and melaena after barium meal showed hiatal hernia [12]. Zullo et al. misdiagnosed a Cameron lesion initially as a neoplastic ulcer [2]. This describes how difficult it can be to make a diagnosis of Cameron lesion if a high index of suspicion is not entertained. Both patients had good outcomes on PPI therapy as established by other studies [2,6]. Erosions were seen on endoscopy of the third patient which was similar to what was obtained on evaluating the first patient. The first patient was however on Amitriptyline which may play a role in the pathology of Cameron lesion as it has been shown to exert an anticholinergic effect on the oesophageal sphincter thereby reducing the tone of the oesophagogastric sphincter, thus aggravating existing hiatus hernia or causing its development [15]. Another study emphasizes the fact that Cameron lesion should be sought even in patients with NSAID use especially when the characteristic lesions of erosions and ulcerations seen with NSAID induced gastrointestinal bleeding are absent [13]. Studies have shown that prognosis is good with long term adequate PPI therapy even if patients have a prior history of PPI therapy [2]. Other modalities of care such as blood transfusion, endoscopic homeostasis and surgery have been described which were not used in the patients discussed as their symptoms resolved completely following the use of PPIs [6,14].
Conclusion
Cameron lesion is an under-recognized cause of upper gastrointestinal bleeding which should be highly suspected in the setting of hiatal hernia. It has good response to PPIs.
Declarations
Conflict of interest statement: The authors have no conflicts of interest to declare.
Ethical consideration: The patients gave oral consent to publish their cases.
Funding sources: None
Informed consent: Informed consent was sought and gotten from the patients.
References
- Chen ZJ. Management of upper gastrointestinal bleeding emergencies: evidence-based medicine and practical consideration. World J Emerg Med. 2011; 2(1): 5. 10.5847/ wjem.j.1920-8642.2011.01.001
- Zullo A, Manta R, De Francesco V et al. Cameron lesions: A still overlooked diagnosis. Case report and systematic review of literature. Clin Res Hepatol Gastroenterol. 2018; 42(6): 604–9. 10.1016/j.clinre.2018.05.002
- Perl D, Leddin D, Bizos D et al. Endoscopic capacity in West Africa. Afr Health Sci. 2016; 16(1): 329. 10.4314/ahs.v16i1.44
- Gray DM, Kushnir V, Kalra G et al. Cameron lesions in patients with hiatal hernias: prevalence, presentation, and treatment outcome. Dis Esophag. 2015; 28(5): 448–452. 10.1111/ dote.12223. Epub 2014 Apr 24.
- Cameron AJ, Higgins JA. Linear gastric erosion. Gastroenterology. 1986; 91(2): 338–342.
- Camus M, Jensen D, Ohning G et al. Severe upper gastrointestinal hemorrhage from linear gastric ulcers in large hiatal hernias: a large prospective case series of Cameron ulcers. Endoscopy. 2013; 45(05): 397–400. 10.1055/s-0032-1326294
- Panzuto F, Di Giulio E, Capurso G et al. Large hiatal hernia in patients with iron deficiency anaemia: a prospective study on prevalence and treatment. Aliment Pharmacol Ther. 2004; 19(6): 663–670. 10.1111/j.1365-2036.2004.01894.x
- Windsor CW, Collis JL. Anaemia and hiatus hernia: experience in 450 patients. Thorax. 1967; 22(1): 73–78. 10.1136/thx.22.1.73
- Katz J, Brar S, Sidhu JS. Histopathological Characterization of a Cameron Lesion. Int J Surg Pathol. 2012; 20(5): 528–530. 10.1177/1066896912446947
- Weston AP. Hiatal Hernia with Cameron Ulcers and Erosions. Gastrointest Endosc Clin N Am. 1996; 6(4): 671–679.
- Smith RE, Shahjehan RD. Hiatal Hernia. 2023.
- Tamene A, Mela M. A large hiatal hernia with cameron ulcer presenting as refractory sever iron deficiency anemia: A case report. J Pediatr Surg Case Rep. 2018; 37: 16–18. 10.1016/j. epsc.2018.07.008
- Seid AS, Mamo EA. Overt GI bleeding from a Cameron lesion in an Ethiopian with NSAID use: Case report of an unusual condition. Ann Med Surg. 2022; 75: 103469. 10.1016/j.amsu.2022.103469
- Nguyen N, Tam W, Kimber R, Roberts-Thomson IC. Gastrointestinal: Cameron’s erosions. J Gastroenterol Hepatol. 2002; 17(3): 343–343. 10.1046/j.1440-1746.2002.02760.
- yber MA. The relationship between hiatus hernia and tricyclic antidepressants: a report of five cases. Am J Psychiatr. 1975; 132(6): 652–653. 10.1176/ajp.132.6.652