
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Optimizing recovery in infraorbital neuropraxia after facial trauma: A case report
Jayasooriya Hk1 *; Abeysinghe AHMGB2 ; Pathirana NPNB1 ; Abeysinghe AHMCD3
1Faculty of Medicine, Wayamba University of Sri Lanka, Sri Lanka.
2Department of Surgery, Faculty of Medicine, Wayamba University of Sri Lanka, Sri Lanka.
3Faculty of Medicine, Rajarata University of Sri Lanka, Sri Lanka.
*Corresponding Author : Jayasooriya Hk
Faculty of Medicine, Wayamba University of Sri
Lanka, Sri Lanka.
Email: kalhara98@gmail.com
Received : Feb 18, 2025
Accepted : Mar 12, 2025
Published : Mar 19, 2025
Archived : www.jcimcr.org
Copyright : © Jayasooriya HK (2025).
Abstract
Background: Infraorbital nerve injury is a common consequence of facial trauma, particularly in zygomatic fractures. The severity of the injury varies, with mild neuropraxia being one of the most common presentations. This case report outlines the clinical management of a patient with infraorbital neuropraxia following a motorcycle accident, emphasizing conservative management and the role of pharmacologic interventions in optimizing recovery.
Case presentation: A 24-year-old male sustained infraorbital neuropraxia after a motorcycle accident. The injury was diagnosed based on clinical findings, imaging studies, and nerve conduction tests. Conservative management with corticosteroids led to significant recovery, as evidenced by the improvement in both clinical symptoms and objective neurophysiological markers.
Conclusion: Infraorbital neuropraxia can be effectively managed conservatively, especially in cases without significant nerve displacement or fractures. Early diagnosis and appropriate treatment, including the use of corticosteroids, can significantly improve outcomes, facilitating nerve recovery and reducing symptoms.
Citation: Jayasooriya Hk, Abeysinghe AHMGB, Pathirana NPNB, Abeysinghe AHMCD. Optimizing recovery in infraorbital neuropraxia after facial trauma: A case report. J Clin Images Med Case Rep. 2025; 6(3): 3515.
Introduction
Infraorbital nerve injury is a prevalent and clinically significant consequence of facial trauma, commonly associated with zygomatic fractures or soft tissue damage, particularly in cases involving direct impact to the midface [1]. The infraorbital nerve, a terminal branch of the maxillary division of the trigeminal nerve, plays a crucial role in providing sensory innervation to key regions of the face, including the cheek, upper lip, and parts of the nasal cavity. Injury to this nerve can lead to a range of sensory disturbances, which vary in severity depending on the extent of the nerve damage [2]. These disturbances can range from mild, transient neuropraxia due to compression, to more severe, irreversible injuries such as nerve avulsion or transection. The severity of sensory disturbances is directly correlated to the extent of the injury, which can be classified according to Sunderland’s classification of nerve injury. This classification categorizes injuries into five distinct grades, ranging from mild neuropraxia (Grade I) to complete nerve transection (Grade V) [3]. In cases of mild neuropraxia (Grade I), often resulting from direct nerve compression or pressure due to surrounding soft tissue swelling, patients typically experience symptoms such as numbness, paresthesia, and a sensation of heaviness over the affected areas, such as the nose and upper lip. In some cases, pain may also be triggered during activities such as chewing, which can further irritate the injured nerve. In more severe cases, such as nerve avulsion or transection, the injury may result in complete anesthesia and dysesthesia, leading to a loss of sensation and altered sensations in the affected region [4-6]. The diagnosis of infraorbital nerve injury primarily relies on clinical examination, which is performed in conjunction with a detailed trauma history. High-resolution imaging techniques, such as facial X-rays and CT scans, can be utilized to assess underlying fractures and soft tissue damage, providing valuable information about the extent of the injury. Electrodiagnostic tests, including Nerve Conduction Studies (NCS) and Electromyography (EMG), can offer objective confirmation of the injury [1,4,7]. These tests measure parameters such as the latency and amplitude of nerve conduction and can help identify the activity of muscles innervated by the affected nerve, thereby aiding in the assessment of nerve function and severity of the injury. The management of infraorbital neuropraxia can be approached using either conservative or surgical methods, depending on the severity of the injury and the presence of additional fractures or complications [1,4]. Both treatment strategies are grounded in the hypothesis that recovery occurs through proximal nerve regeneration or compensatory innervation from nearby sensory nerves, such as the zygomaticofacial and buccal nerves [7]. Conservative management is typically favored for nondisplaced fractures or soft tissue-related nerve injuries, with the goal of alleviating compression and promoting nerve recovery. Treatment options include anti-inflammatory agents, such as corticosteroids, which reduce swelling and inflammation around the nerve, and medications like topiramate, which has shown promise in promoting neural regeneration [1,2]. These medications are administered within a therapeutic range, with dosages carefully titrated based on patient response and functional recovery. In more severe cases of trauma, where there is a risk of ongoing nerve compression due to displaced fractures or other complications, surgical intervention may be required. Surgical management typically involves decompression of the affected nerve through reduction of the zygomatic fracture and mobilization of the nerve and surrounding soft tissues to relieve pressure. Isolated zygomatic fractures are often treated with miniplate fixation via open reduction. Compared to conservative management, surgical intervention offers the advantage of preventing further nerve damage by stabilizing fractured segments and improving the healing process [8]. As a result, surgical treatment may provide superior outcomes in terms of the recovery of sensory function, particularly in cases of significant nerve compression. This case report presents the clinical course of a young male who sustained infraorbital neuropraxia following facial trauma resulting from a motorcycle accident. We detail the diagnostic approach, treatment strategies, and outcomes of conservative management, with a focus on optimizing recovery and enhancing quality of life for patients experiencing similar injuries. By examining this case, we aim to contribute to a deeper understanding of the management of infraorbital neuropraxia and provide insights that can guide clinicians in making informed decisions regarding treatment options and expected outcomes for patients with such injuries.
Case presentation
A 24-year-old male presented to our clinic following a highvelocity head-on collision with another motorcycle while riding as the operator. The impact, which involved significant trauma to the face, neck, and thorax, resulted in substantial facial injuries, predominantly affecting the right side of his face. After the collision, the patient was promptly admitted to the emergency treatment unit. During the initial assessment, he was found to be hemodynamically stable, conscious, and alert. The primary survey confirmed no immediate life-threatening conditions, aside from pain localized to the facial area. Given his stable condition, the patient was subsequently transferred to the surgical ward for further evaluation and management.
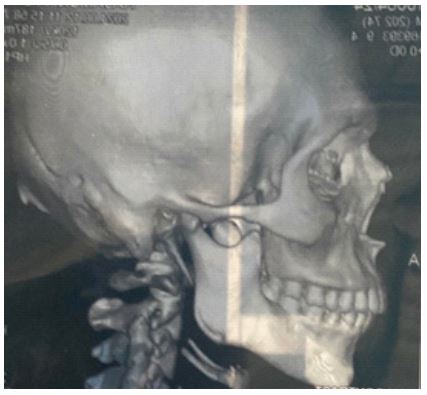
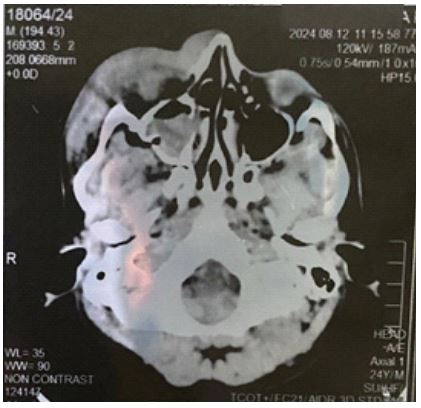
In the ward, the patient reported experiencing moderate paresthesia, numbness, and localized pain in the right cheek, all of which were aggravated by chewing. He described a partial loss of sensation in the affected area, with a notable reduction in his ability to perceive fine touch. Importantly, the patient did not experience any visual disturbances, such as diplopia, nor did he report any signs of bleeding. These findings were reassuring, suggesting that the ocular structures were not directly impacted by the trauma. Based on the clinical presentation, there was concern for a sensory deficit related to the infraorbital nerve, likely resulting from nerve compression due to soft tissue swelling or other post-traumatic changes. Upon initial clinical evaluation, the patient appeared to be in mild distress, particularly when palpating the affected region. Notable tenderness was observed in the right zygomatic region, but there was no evident deformity but extensive soft tissue swelling was noted around the zygomatic region, raising the suspicion of a more subtle fracture. Neurological examination revealed a sensory deficit, with impaired fine touch and two-point discrimination over the area corresponding to the distribution of the infraorbital nerve. These findings were highly indicative of a neuropraxia, likely resulting from compression of the infraorbital nerve by the surrounding soft tissue edema and hematoma. To confirm the extent of the injury and rule out other potential complications, the patient was immediately subjected to imaging studies. As an initial investigation, a facial X-ray was performed, given its accessibility and utility in identifying skeletal fractures. The X-ray revealed a zygomatic fracture, raising concern for possible nerve involvement. Subsequently, a noncontrast CT scan of the face was carried out, which ruled out any intracranial injuries. The CT scan further demonstrated a zygomatic bone fracture; however, there was no displacement or associated fractures of the orbital floor, which was reassuring. Additionally, the imaging revealed a maxillary sinus hematoma and extensive soft tissue edema in the region surrounding the affected zygomatic bone. Further evaluation, including 3D reconstruction of the CT images, excluded any significant displacement of the fracture, confirming that surgical intervention was not necessary at this stage. To objectively assess the functional status of the infraorbital nerve, a nerve conduction test was performed the day after the injury. The test revealed notable impairment in the sensory nerve conduction of the infraorbital nerve, with a latency of 2.2 ms and an amplitude of 27.3 mV, consistent with the clinical suspicion of neuropraxia. Given the absence of displaced fractures and the confirmed diagnosis of infraorbital neuropraxia, it was determined that the patient’s symptoms were most likely attributed to nerve compression caused by the surrounding edema and hematoma. Consequently, a conservative management approach was initiated, aimed at alleviating pressure on the nerve and promoting recovery. The treatment regimen included the administration of intravenous dexamethasone to reduce inflammation and manage swelling in the affected area. After 24 hours, the patient was transitioned to oral methylprednisolone to continue addressing inflammation and support recovery. This pharmacologic strategy was intended to minimize the impact of soft tissue edema on the infraorbital nerve and facilitate nerve healing by reducing pressure and promoting regeneration. Over the course of subsequent follow-up visits, the patient demonstrated both subjective and objective improvement in his symptoms. His reports of paresthesia and numbness gradually diminished, and objective improvement was noted in the nerve conduction studies. The latency decreased to 2.8 ms, and the amplitude improved to 32.6 mV, suggesting positive progression in nerve function. These findings were consistent with the clinical resolution of the neuropraxia and further reinforced the efficacy of the conservative management approach in promoting nerve recovery. In summary, the patient’s recovery was marked by a substantial reduction in symptoms and improved nerve conduction, indicative of successful conservative management. This case illustrates the importance of early diagnosis, objective neurophysiological testing, and a tailored treatment strategy in optimizing outcomes for patients with infraorbital neuropraxia following facial trauma.

Discussion
Infraorbital neuropraxia is a significant clinical consequence of facial trauma, with zygomatic fractures being a common cause. The infraorbital nerve, a branch of the maxillary division of the trigeminal nerve, provides sensory innervation to regions of the face, including the cheek, upper lip, and parts of the nasal cavity [1]. When the nerve is injured, the resulting symptoms can range from mild numbness and paresthesia to complete anesthesia in the affected area [4-6]. The severity of the injury can be classified according to Sunderland’s classification, with neuropraxia representing the least severe form, characterized by temporary impairment due to nerve compression [3]. In this case, the patient’s injury was consistent with Grade I neuropraxia (mild compression), as the clinical findings of numbness and altered sensation were accompanied by tenderness in the zygomatic region but no other signs of severe injury, such as diplopia or ocular involvement [1,2]. Imaging studies confirmed a zygomatic fracture with soft tissue swelling but no displacement or involvement of the orbital floor, which further supports the diagnosis of a mild neuropraxia resulting from nerve compression [7]. Electrodiagnostic tests, including Nerve Conduction Studies (NCS), are crucial in confirming the diagnosis and assessing the degree of nerve damage [4,5]. In our case, the initial NCS showed a delayed latency and reduced amplitude, consistent with neuropraxia, which improved with conservative management. These findings align with previous studies that demonstrated the utility of NCS in evaluating infraorbital nerve injuries and monitoring recovery [5]. Additionally, sensory testing, such as two-point discrimination, was instrumental in assessing the functional impairment of the nerve, confirming the presence of a sensory deficit in the affected region. The management of infraorbital neuropraxia typically includes conservative measures, particularly for mild to moderate injuries. As reported in the literature, corticosteroids such as dexamethasone and methylprednisolone are commonly used to reduce inflammation around the nerve, thereby promoting recovery [2-7]. In our case, the patient showed significant improvement after receiving corticosteroid therapy, with a notable reduction in symptoms and improvement in nerve conduction, demonstrating the efficacy of this treatment approach. Similar findings were reported by Vriens et al. (1998), who noted the positive impact of anti-inflammatory agents in enhancing nerve regeneration following trauma [2]. While conservative management is effective for many patients, surgical intervention may be indicated for more severe cases, such as those involving nerve transection or extensive fracture displacement [8]. However, as shown in this case, the absence of significant fracture displacement and the early use of corticosteroids resulted in a favorable outcome without the need for surgery. This case underscores the importance of early diagnosis and timely intervention in optimizing recovery from infraorbital neuropraxia. By utilizing clinical evaluation, neurophysiological testing, and conservative treatment, significant recovery can be achieved in most patients, as demonstrated in this case.
Conclusion
Infraorbital neuropraxia is a common sequela of facial trauma, particularly following zygomatic fractures. Early diagnosis, supported by imaging and nerve conduction studies, is essential for determining the appropriate management strategy. Conservative treatment, including the use of corticosteroids to reduce inflammation and promote nerve regeneration, can lead to significant improvement in symptoms and nerve function. Surgical intervention may be required for more severe injuries, but in cases of mild neuropraxia, conservative management is often sufficient. This case highlights the importance of individualized treatment plans and the role of neurophysiological monitoring in optimizing recovery outcomes for patients with infraorbital neuropraxia.
Declarations
Acknowledgment: The authors would like to express their gratitude to the patient for providing consent to share this case and to the medical and surgical teams at the Faculty of Medicine, Wayamba University of Sri Lanka, for their invaluable contributions to patient care and data collection. We also extend our appreciation to the Department of Radiology for their assistance in imaging studies and interpretation.
Conflict of interest: The authors declare no conflicts of interest related to this case report. No financial or material support was received that could have influenced the findings or conclusions of this study
References
- Lone PA, Singh RK, Pal US. Treatment of traumatic infra orbital nerve paresthesia. Natl J Maxillofac Surg. 2012; 3(2): 218-9.
- Vriens JP, van der Glas HW, Bosman F, Koole R, Moos KF. Information on infraorbital nerve damage from multitesting of sensory function. Int J Oral Maxillofac Surg. 1998; 27(1): 20-6.
- Peripheral nerve regeneration and intraneural revascularization - PMC [Internet] 2025. https://pmc.ncbi.nlm.nih.gov/articles/ PMC6263011/.
- Lee SY, Kim SH, Hwang JH, Kim KS. Sensory recovery after infraorbital nerve avulsion injury. Arch Craniofacial Surg. 2020; 21(4): 244-8.
- Hong WT, Choi J hee, Kim JH, Kim YH, Yang CE, et al. Trigeminal somatosensory evoked potential test as an evaluation tool for infraorbital nerve damage. Arch Craniofacial Surg. 2019; 20(4): 223-7.
- Ohki M, Takeuchi N. Objective evaluation of infraorbital nerve involvement in maxillary lesions by means of the blink reflex. Arch Otolaryngol Head Neck Surg. 2002; 128(8): 952-5.
- Compensatory alterations in dermal innervations in patients with congenital insensitivity to pain [Internet]. 2025. https:// www.healthdisgroup.us/articles/GJRD-4-118.php.
- Iro H, Bumm K, Waldfahrer F. Rehabilitation of the trigeminal nerve. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2005; 4: 12.