
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Bright fornix in Wernicke’s encephalopathy
Somarajan Anandan1 *; Caroline Surendran Pushpaletha2
1Department of Neurology, St Joseph Hospital, Anchal, Kollam, Kerala, India.
2Department of Medicine, St Joseph Hospital, Anchal, Kerala, India.
*Corresponding Author : Somarajan Anandan
Department of Neurology, St Joseph Hospital,
Anchal, Kerala, India.
Email: drsomarajan@yahoo.co.in
Received : Feb 17, 2025
Accepted : Mar 12, 2025
Published : Mar 19, 2025
Archived : www.jcimcr.org
Copyright : © Anandan S (2025).
Citation: Anandan S, Surendran Pushpaletha C. Bright fornix in Wernicke’s encephalopathy. J Clin Images Med Case Rep. 2025; 6(3): 3516.
Description
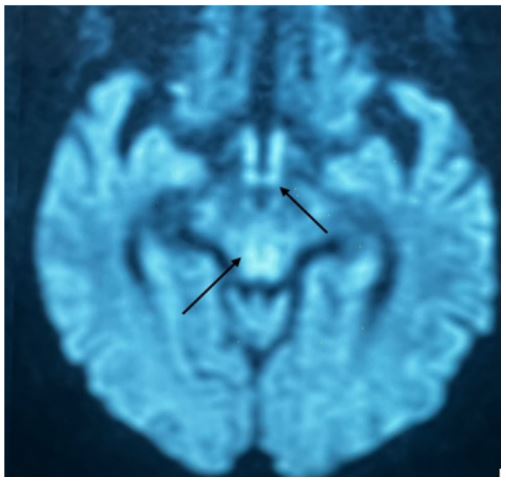
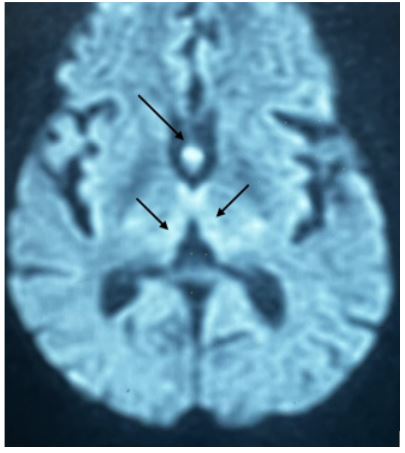
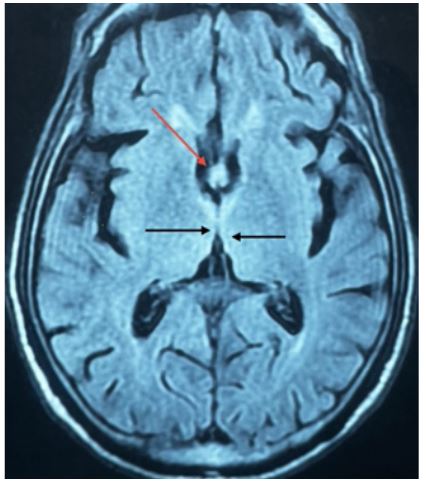
A 70-year-old man with parkinsonism presented with altered sensorium of 3 days duration. He had a history of fever and cough one week back and was admitted in local hospital and had several intravenous fluid infusions. There was no history of alcohol intake. His only medication was levodopa/carbidopa. He has a history of poor food intake since several weeks. On examination he was drowsy and had bilateral external ophthalmoplegia and gaze evoked nystagmus. There was no limb weakness or limb incoordination. Magnetic resonance imaging of brain showed hyperintensity of bilateral paramedian thalamus, mamillary body, periaqueductal region and pons. In addition, fornix showed hyperintensity in diffusion weighted image and fluid attenuated inversion recovery images (Bright Fornix) (Figures 1-3). There was no diffusion restriction. Wernicke’s encephalopathy is an acute neuropsychiatric disorder resulting from thiamine deficiency and is characterized by a clinical triad of confusion, ocular abnormalities, and ataxia. Only 16% of patients show full clinical triad and 19% of patients have none of these signs [1]. Thiamine deficiency causes dysfunction of the Krebs cycle and the pentose phosphate pathway. Magnesium is a necessary cofactor for the conversion of thiamine into its active form, Thiamine Diphosphate (TDP). Magnetic Resonance Imaging (MRI) typically shows bilaterally symmetrical lesions in the paraventricular regions of the thalamus, hypo thalamus, mammillary bodies, periaqueductal region and floor of the fourth ventricle. MRI may also show unusual sites of brain lesions such as the putamen, caudate, splenium of the corpus callosum, dorsal medulla, pons, red nucleus, substantia nigra of the midbrain, cranial nerve nucleus, vermis, dentate nucleus, paravermian region of the cerebellum, fornix and pre- and postcentral gyri [2]. Involvement of white matter tracts such fornix is only rarely reported [3].
References
- Harper CG, Giles M, Finlay-Jones R. Clinical signs in the Wernicke-Korsakoff complex:A retrospective analysis of 131 cases diagnosed at necropsy. J Neurol Neurosurg Psychiatry. 1986; 49(4): 341-5. doi: 10.1136/jnnp.49.4.341.
- Zuccoli G, Pipitone N. Neuroimaging findings in acute Wernicke’s encephalopathy: Review of the literature. AJR Am J Roentgenol. 2009; 192: 501-8. 10.2214/AJR.07.3959.
- RS Borges, N Ventura, EL Gasparetto, MVR Pinto. Forniceal Involvement in Wernicke Encephalopathy American Journal of Neuroradiology. 2011; 32 (11): 209. DOI: 10.3174/ajnr. A2888.