
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
A rare case of uterine hydatid cyst in disseminated hydatidosis
Sachin Khanduri; Avani Kanojia*; Aniket Chugh; Aastha Agrawal; Sana
Department of Radiodiagnosis, Era’s Lucknow Medical College and Hospital, Lucknow, India.
*Corresponding Author : Avani Kanojia
Department of Radiodiagnosis, Era’s Lucknow
Medical College and Hospital, Lucknow, India.
Email: avanikanojia1997@gmail.com
Received : Feb 18, 2025
Accepted : Mar 13, 2025
Published : Mar 20, 2025
Archived : www.jcimcr.org
Copyright : © Kanojia A (2025).
Abstract
Hydatid disease, caused by Echinococcus species, primarily affects the liver and lungs but can occasionally involve unusual anatomical locations. We report a rare case of disseminated hydatidosis in a middleaged female with an atypical hydatid cyst embedded within the posterior uterine wall. The diagnostic challenge posed by the cystic lesion in the recto-uterine pouch underscores the importance of multimodal imaging in identifying uncommon presentations of the disease.
Keywords: Hydatid disease; Uterine hydatid cyst; Atypical hydatidosis; Posterior uterine wall; CT imaging.
Citation: Khanduri S, Kanojia A, Chugh A, Agrawal A, Sana. A rare case of uterine hydatid cyst in disseminated hydatidosis. J Clin Images Med Case Rep. 2025; 6(3): 3517
Introduction
Echinococcus is a parasitic worm with four forms that named Echinococcus granulosus, E. multilocularis, E. vogeli and E. oligarthrus. Disease that made by this parasite (mostly by E. granulosus) was named Hydatidosis (Echinococcosis) [1]. E. granulosus has lifespan of 5-20 month. This tapeworm’s long is 5 mm. Its definitive host is canids, mostly dogs. Echinococcus grows up in intestine (jejunum) and releases the eggs. Eggs excreted with the feces and ingested by intermediate hosts (sheep, cattle, pigs, horses, camels and humans) [2]. The liver (75%) and lungs (15%) are the most commonly affected organs, with extrahepatic dissemination being rare. Genital tract involvement is extremely uncommon, accounting for less than 0.5% of reported cases. Here, we describe an unusual case of hydatid disease with disseminated hepatic and peritoneal involvement, along with an atypical hydatid cyst embedded in the posterior uterine wall, highlighting its diagnostic and surgical implications.
Case presentation
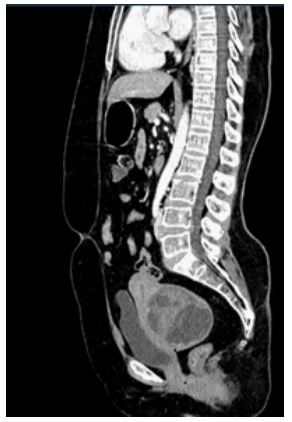
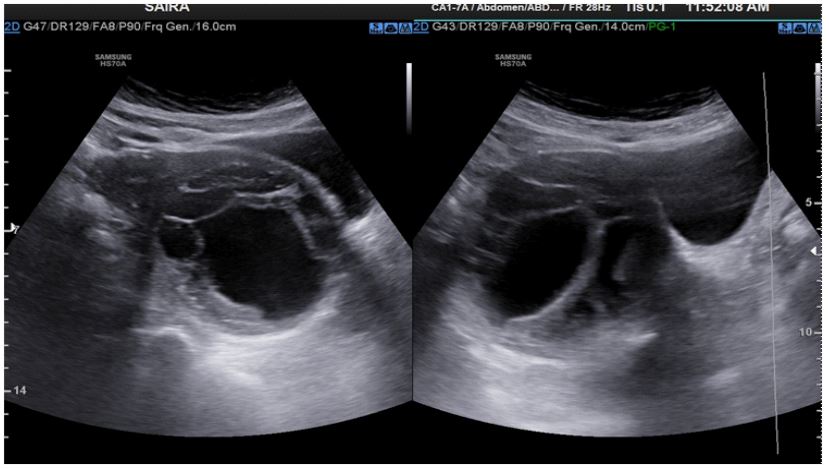
A 45-year-old female presented with chronic, nonspecific abdominal pain and secondary infertility, with no history of previous surgeries, trauma, or known parasitic infections. Physical examination was unremarkable, with no palpable abdominal masses or organomegaly. Ultrasound revealed multiple cystic lesions in the hepatic and peritoneal regions, suggestive of disseminated hydatidosis, along with a distinct cystic lesion in the recto-uterine pouch, posing a diagnostic challenge. Computed Tomography (CT) scan identified a well-demarcated cystic lesion within the posterior uterine wall, an unusual finding given the rarity of hydatid disease involving the myometrium, with no signs of calcification or daughter cysts. Serological testing through Enzyme-Linked Immunosorbent Assay (ELISA) for Echinococcus antibodies was positive.



Discussion
While hepatic and peritoneal hydatidosis is well-documented, involvement of the uterus is exceedingly rare. The most plausible explanation for this dissemination is hematogenous or lymphatic spread from a primary hepatic focus. The differential diagnosis for uterine cystic lesions includes müllerian cysts, endometriotic cysts, and degenerated fibroids, making definitive preoperative diagnosis challenging. This case underscores the importance of considering hydatid disease in the differential diagnosis of cystic lesions in endemic regions.
Albendazole may serve as a therapeutic option alongside surgical and percutaneous treatment [3]. It is not recommended as a first-line treatment and is generally avoided during pregnancy, particularly in the first trimester, due to the risk of teratogenicity [4]. Timely surgical intervention for pelvic cysts leading to obstructive uropathy can help prevent further renal damage [5].
Conclusion
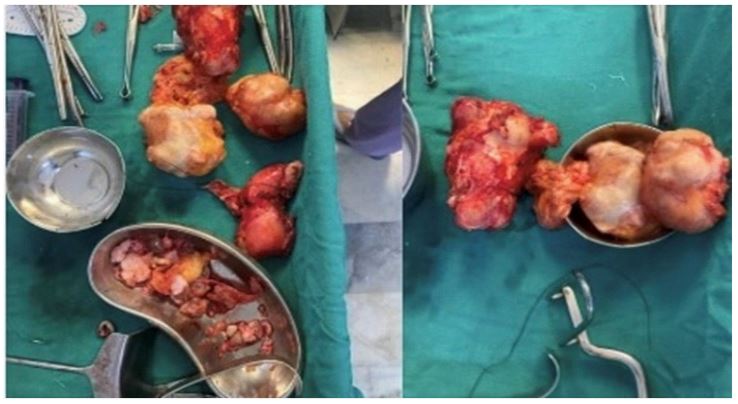
This case highlights an atypical presentation of disseminated hydatidurias with a rare uterine hydatid cyst, emphasizing the need for a high index of suspicion and multimodal imaging for accurate diagnosis. Surgical excision remains the mainstay of treatment, complemented by antiparasitic therapy to minimize recurrence.
References
- Başgül A, Kavak ZN, Gökaslan H, & Küllü S. Hydatid cyst of the uterus. Infectious diseases in obstetrics and gynecology. 2002; 10(2): 67.
- Görgen H, Api M, Çetin A. Primary adnexial hydatid cyst mimicking ovarian tumor. Journal of the Turkish German Gynecological Association. 2009; 10(4): 232.
- Peyvandi S, Zamaniyan M, Rahmani Z, Hoseini S. Conservative treatment of hydatid cyst in pregnancy: Case report. J Genit Syst Disord. 2017; 6: 1.
- Gyorkos TW, St-Denis K. Systematic review of exposure to albendazole or mebendazole during pregnancy and effects on maternal and child outcomes, with particular reference to exposure in the first trimester. Int J Parasitol. 2019; 49(7): 541-54.
- Yağmur I, Kocaman OH, Dere O, Demir M, Katı B, et al. Multiorgan echinococcosis with uterine involvement causing bilateral hydronephrosis in a child: case report. Iran J Parasitol. 2022; 17(3): 425-43.