
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Persistent mediastinal chylothorax following surgical pulmonary vein isolation
Marcus Taylor1 *; Joshua Halyckyj-Smith2 ; David Rose1 ; Gianluca Lucchese3
1Department of Cardiac Surgery, Blackpool Victoria Hospital, Blackpool, UK.
2Department of Cardiac Surgery, Manchester University NHS Foundation Trust, Manchester, UK.
3Department of Cardiac Surgery, St. Thomas’ Hospital, London, UK.
*Corresponding Author : Marcus Taylor
Department of Cardiac Surgery, Blackpool Victoria
Hospital, Blackpool, UK.
Tel: 00447910538817;
Email: marcus.taylor1@nhs.net
Received : Feb 26, 2025
Accepted : Mar 14, 2025
Published : Mar 21, 2025
Archived : www.jcimcr.org
Copyright : © Taylor M (2025).
Abstract
This case describes persistent mediastinal chylothorax following bioprosthetic aortic valve replacement and concomitant pulmonary vein isolation for atrial fibrillation. The chylothorax persisted for more than 30 days after surgery and resolved after lymphangiography. To the best of our knowledge, this is the sole published case reporting mediastinal chylothorax caused by of pulmonary vein isolation.
Keywords: Chylothorax; Pulmonary vein isolation; Atrial fibrillation.
Citation: Taylor M, Halyckyj-Smith J, Rose D, Lucchese G. Persistent mediastinal chylothorax following surgical pulmonary vein isolation. J Clin Images Med Case Rep. 2025; 6(3): 3519.
Introduction
We report the case of mediastinal chylothorax following bioprosthetic aortic valve replacement and concomitant Pulmonary Vein Isolation (PVI) for atrial fibrillation. The procedure was carried out via median sternotomy. PVI was performed by applying a bipolar radiofrequency clamp (AtriCure Synergy Series, AtriCure, Inc., Cincinnati, OH) to the surrounding cuff of atrial tissue. After an initial uncomplicated post-operative course, on the 2nd Post-Operative Day (POD) the fluid draining from the mediastinal drain turned from serous to a pale white, raising the clinical suspicion of chylothorax. The diagnosis was confirmed with biochemical analysis of the fluid that revealed a total triglyceride count of 315.04 mg/dL. The average drainage was 500-600 mL per day and hence the mediastinal drain was kept in place. Initially, the patient was managed with a lipidic diet, but considering the poor compliance of both the patient and kitchen, he was switched to Total Enteral Nutrition (TEN) via a Nasogastric (NG) tube and received a low-fat diet rich in Medium-Chain Fatty Acids (MCFA). Despite this, there was still no reduction in the amount of fluid drained over the next 72 hours. Next, intravenous somatostatin (octreotide) was started at a dose of 200 μg three times daily for the first 48 hours, reduced to 100 μg three times daily for the next seven days. By POD 18, the mediastinal drainage had decreased considerably. Therefore, the drain was clamped, and the patient was gradually restarted on an oral low-fat diet. A transthoracic echocardiogram performed 12 hours after clamping revealed a global pericardial effusion of 2-3 cm and hence the drain was unclamped to allow the fluid to drain. The patient’s NG feed was subsequently recommenced and investigations to visualize the leak were undertaken. A lymphangiogram was carried out by performing an ultrasound-guided right inguinal lymph node puncture and infiltration with 10 mls of iodinated poppy-seed oil followed by a Computed Tomography (CT) scan. Whilst a small area of contrast pooling in the anterior mediastinum was seen on CT, there was no clear evidence of a major leak (Figure 1). Within the next 24-48 hours the volume of fluid draining began to reduce significantly. On POD 34 the patients were restarted on an oral low-fat oral diet. The fluid volume continued to decrease, and the mediastinal chest drain was removed on POD 38. Subsequent transthoracic echocardiogram and chest radiography did not indicate re-accumulation of fluid. The patient was discharged home on POD 40. At his 1-year follow-up examination he remained well, with no recurrence of mediastinal collection.
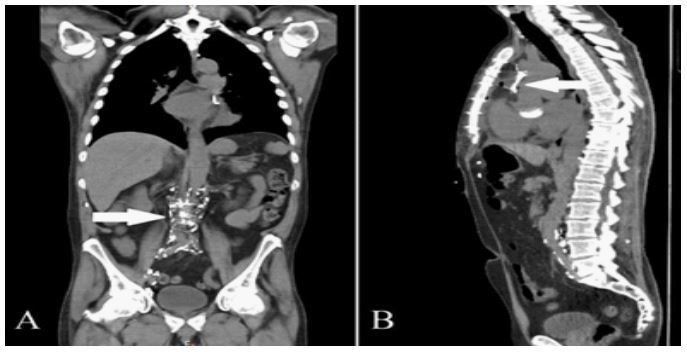
Panel A: Coronal view showing opacification of the lymphatic tree in the expected paraaortic route (arrow) following contrast injection into the right inguinal lymph node.
Panel B: Sagittal view showing a small area of contrast (arrow) pooling in the anterior mediastinum (with an air fluid level present). No clear evidence of leak.
Discussion
Chylothorax is a rare complication of cardiac surgery. It has a reported prevalence of 0.3% to 1.5% and is most frequently seen after iatrogenic injury of the lymphatic duct during harvesting of the Left Internal Mammary Artery (LIMA). Post-operative chylothorax is associated with high rates of morbidity and mortality [1]. It can cause metabolic disturbances, nutritional deficiencies, respiratory disorders, immunodeficiency and infections. It also causes prolonged hospitalisation, higher treatment costs, and has a negative psychological effect on patients, particularly when management involves an absence of enteral nutrition. To the best of our knowledge, this is the only reported case whereby the damage to lymphatic structures and subsequent pericardial chylothorax (in the absence of LIMA harvesting) was presumed to have occurred during PVI. Due to the fact that both pleurae were intact, the fluid accumulated into the mediastinum, resulting in a pericardial effusion. Different anatomical variants of lymphatic structures are common and hence we postulate that in this scenario there was most likely injury to thoracic duct tributaries at the time of PVI. The established literature supports an initial trial of conservative management with a low-fat diet. Somatostatin should be considered when dietary adjustments fail to resolve the issue. Surgical intervention is considered only when conservative treatments have failed. In this case diagnostic lymphangiography alone resulted in successful treatment of the chylothorax [2]. The mechanism by which lymphangiography reduces chyle leaks remains unclear, although some authors have suggested that the inflammatory and granulomatous reaction effect of contrast agents injected at the time of lymphangiography can cause tissue necrosis or pulmonary artery embolization [3]. This case has described successful management of the rare yet serious complication of post-operative chylothorax after cardiac surgery.
Declarations
Funding: No funding was received for this work.
Conflict of interest: None declared.
Data availability: Due to the risk of patient identification, data cannot be shared.
Ethical statement: Informed verbal consent was obtained from the patient.
References
- Cerfolio RJ, Allen MS, Deschamps C, Trastek VF, Pairolero PC. Postoperative chylothorax. J Thorac CardiovascSurg. 1996; 112(5): 1361-5.
- Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardiothorac Surg. 2016; 49(1): 18-24.
- Porziella V, Cesario A, Margaritora S, Granone P. Role of preoperative lymphangiogram and lympangioscintigraphy in the surgical management of spontaneous chylothorax. Eur J Cardiothorac Surg. 2006; 30(5): 813.