
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
Surgical management of giant coronary artery to pulmonary artery fistula aneurysm
Omar Bittar1 ; Marcus Taylor2 *; Sharath Hosmane3 ; Mohamad N Bittar2
1Manchester Medical School, University of Manchester, Manchester, UK.
2Department of Cardiac Surgery, Blackpool Victoria Hospital, Blackpool, UK.
3Department of Radiology, Royal Preston Hospital, Preston, UK.
*Corresponding Author : Marcus Taylor
Department of Cardiac Surgery, Blackpool Victoria
Hospital, Blackpool, UK.
Tel: 00447910538817;
Email: marcus.taylor1@nhs.net
Received : Feb 26, 2025
Accepted : Mar 14, 2025
Published : Mar 21, 2025
Archived : www.jcimcr.org
Copyright : © Taylor M (2025).
Abstract
A 74-year-old female presented with mild exertional shortness of breath and pain between her shoulder blades on a background of chronic cough and occasional haemoptysis. Chest radiography demonstrated an abnormal bulge over the left heart border and subsequent dedicated cardiac computed tomography confirmed the presence of a 35 mm aneurysmal fistula between a high septal branch of the left anterior descending coronary artery and the root of the main pulmonary artery. The patient underwent surgery, during which the aneurysm was opened and obliterated with a double layer of 4-0 prolene. The procedure was uneventful, and the patient recovered well. She was discharged home on the sixth post-operative day and remains alive and well at the time of writing. Coronary artery to pulmonary artery fistula aneurysm is a rare pathology. Diagnosis can be difficult due to the varying possibilities of presentation. These include as an incidental finding, presenting with mild symptoms or with cardiovascular collapse due to rupture. Symptom burden is associated with aneurysm size and degree of shunt. Given the risk of rupture, surgery is recommended for all aneurysms, especially those large in size and presenting with symptoms.
Keywords: Coronary artery; Pulmonary artery; Fistula; Aneurysm; Cardiopulmonary bypass.
Citation: Bittar O, Taylor M, Hosmane S, Bittar MN. Surgical management of giant coronary artery to pulmonary artery fistula aneurysm. J Clin Images Med Case Rep. 2025; 6(3): 3520
Case report
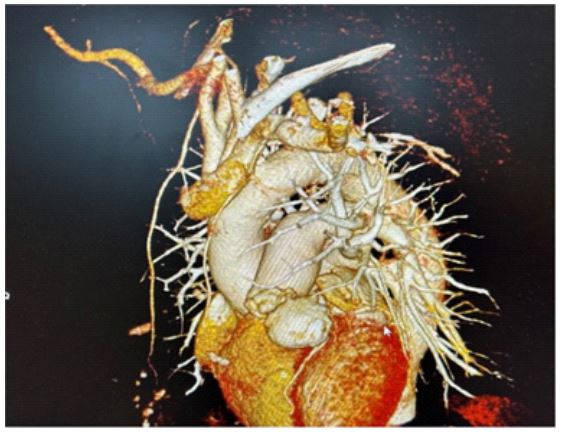
A 74-year-old female presented with mild exertional shortness of breath and pain between her shoulder blades on a background of chronic cough and occasional haemoptysis. Past medical history included previous smoking history, hypertension, insulin dependent diabetes mellitus, raised body mass index and mild bronchiectasis. Chest radiography demonstrated an abnormal bulge over the left heart border. Computed Tomography (CT) of the thorax showed no suspicious parenchymal pathology but raised the possibility of a fistulous communication between the Left Anterior Descending (LAD) coronary artery and the main Pulmonary Artery (PA). A subsequent dedicated cardiac CT confirmed the presence of a 35 mm aneurysmal fistula between a high septal branch of the LAD and the root of the main PA (draining into the left lateral side) as shown in (Figure 1). The main PA was not dilated. Coronary angiography showed significant flow-limiting lesions in the LAD and Circumflex (Cx) coronary arteries.
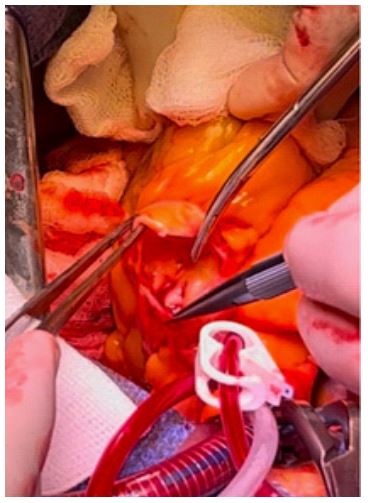
After discussion at a multidisciplinary team meeting, the patient was referred for surgical intervention and latterly underwent surgery via median sternotomy with the use of Cardiopulmonary Bypass (CPB) (CPB time 100 minutes and cross-clamp time 82 minutes). The aneurysm was calcified on the medial and lateral walls but had a very thin anterior wall. The feeding vessel from the LAD and the point of drainage into the PA were both double ligated. The aneurysm was opened (Figure 2), the walls were partially excised, and the aneurysm sac was obliterated with a double layer of 4-0 prolene. Concomitant coronary artery bypass grafting to the LAD and Cx arteries was also performed. The procedure was uneventful, and the patient recovered well. She was discharged home on the sixth post-operative day and remains alive and well at the time of writing.
Discussion/conclusion
Coronary Artery to Pulmonary Artery (CAPA) fistulae are rare, with an incidence of less than 0.5% in the general population. Whilst aneurysm formation is present in approximately 25% of cases, aneurysm size exceeding 30 mm (as seen in this case) has seldom been reported [1]. The majority (>80%) of CAPA fistulae drain into the left lateral side of the main PA [2]. However, origination of the fistula from a septal branch rather than the LAD proper (as seen in this case) is not well described in the literature. Although small aneurysms are usually asymptomatic and detected incidentally, larger aneurysms can present with chest pain or shortness of breath, with severity of symptoms associated with increased volume of shunt or the presence of coronary steal. Alternatively, patients can present with collapse or cardiovascular compromise secondary to leak or rupture of the aneurysm [3]. Due to the risk of rupture, surgical treatment is usually recommended, especially for large aneurysms. However, some studies do report success with a conservative approach [4]. This case report details efficient multidisciplinary working to facilitate prompt diagnosis and management of an exceptionally large CAPA fistula aneurysm after presentation with non-specific symptoms [5]. Surgery can be safely undertaken and should be considered for all patients with acceptable surgical risk in order to mitigate the life-threatening consequences associated with aneurysm rupture.
Declarations
Funding statement: No funding was received for this work.
Conflict of interest statement: of interest: none declared.
Data availability statement: Data is available upon reasonable request.
Ethical statement: Informed written consent has been obtained from the patient.
Author contribution statement
Conceptualisation: MNB.
Data curation: OB.
Formal analysis: MT
Supervision: MNB.
Writing (original draft): OB, MT
Writing (review and editing): All authors
References
- Yun G, Nam TH, Chun EJ. Coronary Artery Fistulas: Pathophysiology, Imaging Findings, and Management. Radiographics 2018; 38: 688-703.
- Hirofuji A, Furugen A, Kamada T, et al. Giant Coronary Aneurysm with Coronary-Pulmonary Artery Fistula in a Jehovah’s Witness. The Thoracic and Cardiovascular Surgeon Reports 2023; 12: 1.
- Angelini P. Coronary-to-Pulmonary Fistulae: What Are They? What Are Their Causes? What Are Their Functional Consequences? Texas Heart Institute Journal. 2000; 27: 327.
- Hijikata S, Sakurai K, Maeba S, et al. Cardiac tamponade due to ruptured coronary-pulmonary artery fistula aneurysm: a case report. European Heart Journal. 2020; 4: 1.
- Seitz A, Schäfer S, Backes M, et al. Giant Aneurysm of a Coronary-Pulmonary Artery Fistula: A Rare Cause of a Diastolic Murmur. Cardiovascular Innovations and Applications. 2019; 4: 143.