
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Chronic sigmoid adult intussusception secondary to quiescent longstanding diverticula
Casey Marie DeBeltz1 ; Clive Jude Miranda1 *; Fnu Monik2 ; Marcellus Anthony Singh1 ; Robert Thomas Kizer1
1Department of Gastroenterology, CHI Health Creighton University Medical Center - Bergan Mercy, Omaha, NE, United States.
2Department of Pathology, CHI Health Creighton University Medical Center - Bergan Mercy, Omaha, NE, United States.
*Corresponding Author : Clive J Miranda
CHI Health Creighton University Medical Center -
Bergan Mercy 7500 Mercy Rd Omaha, NE 68124,
USA.
Tel: (202) 812-8424;
Email: clive.miranda91@gmail.com
Received : Feb 17, 2025
Accepted : Mar 18, 2025
Published : Mar 25, 2025
Archived : www.jcimcr.org
Copyright : © Miranda CJ (2025).
Abstract
Chronic large bowel intussusception in adults in rare with literature limited to scattered case reports. The majority of intussusception occurs in pediatric populations and in the small bowel with etiologies ranging from malignancy to polyps. Here we present a case of a middle-aged female presenting with chronic sigmoid intussusception from a history of prior recurrent diverticular disease which required surgical intervention. This aims to highlight that diverticular disease, even in the absence of a flare, is an uncommon but notable etiology of adult colonic intussusception.
Citation: DeBeltz CM, Miranda CJ, Monik F, Anthony Singh M, Kizer RT. Chronic sigmoid adult intussusception secondary to quiescent longstanding diverticula. J Clin Images Med Case Rep. 2025; 6(3): 3523.
Description
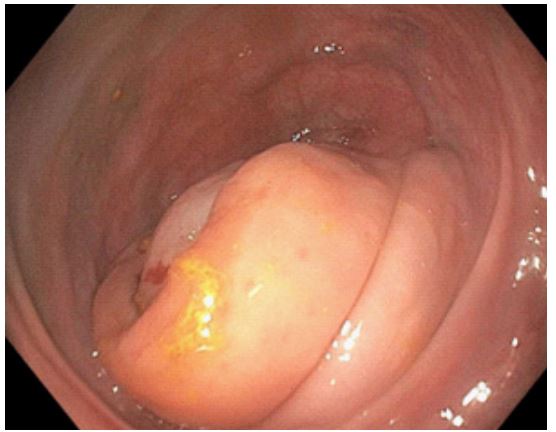
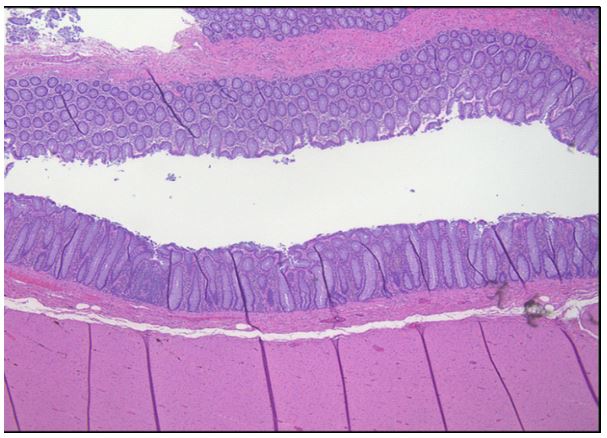
A 54-year-old female with a remote history of recurrent uncomplicated diverticulitis presented with worsening nausea and abdominal pain. Initial computed tomography (CT) scan was concerning for a sigmoid “stricture” with proximal colonic distention, similar to imaging from several years prior. Repeat CT with rectal gastrografin revealed a characteristic stenotic “apple core lesion” suspicious for a malignancy (Figure 1) but no inflammation concerning for enteritis or colitis. She underwent an inpatient colonoscopy which demonstrated congested mucosa and telescoping of the lumen in the mid-sigmoid colon consistent with a sigmoid intussusception without fixed stenosis or stricture (Figure 2). Mucosa from this area was biopsied and was negative for inflammatory changes or malignancy (Figure 3). Of note, a colonoscopy four years prior with biopsy of that area of interest had similar findings. Because of recurrent prior presentations for diverticulitis and abdominal discomfort, the patient underwent a sigmoid colectomy with diverting loop ileostomy. She was found to have intrabdominal adhesions and several fibrotic nodules and scarring on the outer surface of the colon. Surgical pathology showed multiple chronic diverticula without active inflammation or malignancy. Adults comprise only ~5% of cases of bowel intussusception, with most cases occurring in the small bowel with etiologies predominantly secondary to polyps, malignancy, or inflammatory lesions [1]. There are only scattered case reports of adult colonic intussusception from due to diverticula but notably these are from complications such as intraluminal stricture, active diverticulitis, or inverted diverticula [2-4]. Our case is unique due to the absence of active diverticulitis or intraluminal complications of diverticular disease, and illustrates a rare phenomenon of quiescent diverticula as a lead point for chronic sigmoid intussusception.

Declarations
Conflict of interest statement: The authors declare that they have no conflicts of interest.
Ethical principles/informed consent statement: Informed consent was obtained from the patient for the publication of their information and imaging.
Funding: No funding was obtained for this study
References
- Marinis A, Yiallourou A, Samanides L, et al. Intussusception of the bowel in adults: a review. World J Gastroenterol. 2009; 15(4): 407-411.
- Syed H, Syed L, Parampalli U, et al. Adult intussusception secondary to diverticular disease. BMJ Case Rep. 2018. doi: 10.1136/ bcr-2018-226678.
- Oyama T, Akagi T, Etoh T, et al. Intussusception in the ascending colon caused by cecal chronic diverticulitis: a case report. J Surg Case Rep. 2022; (5). doi:10.1093/jscr/rjac204
- Zhang B, Wang J, Li X, et al. Intussusception caused by an inverted colonic diverticulum: a case report. J Med Case Rep. 2018; 12(1): 114. doi:10.1186/s13256-018-1652-9