
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 6
A case of rapidly progressive encephalopathy with bilateral symmetrical deep grey matter involvement: A diagnostic dilemma
*Corresponding Author : Surendra Khosya, MBBS, MD, DM (Neurology)
Associate Director Neurology, Eternal Hospital,
Jaipur, Rajasthan, India.
Email: drkhosya3@gmail.com
Received : Feb 17, 2025
Accepted : Mar 19, 2025
Published : Mar 26, 2025
Archived : www.jcimcr.org
Copyright : © Khosya S (2025).
Abstract
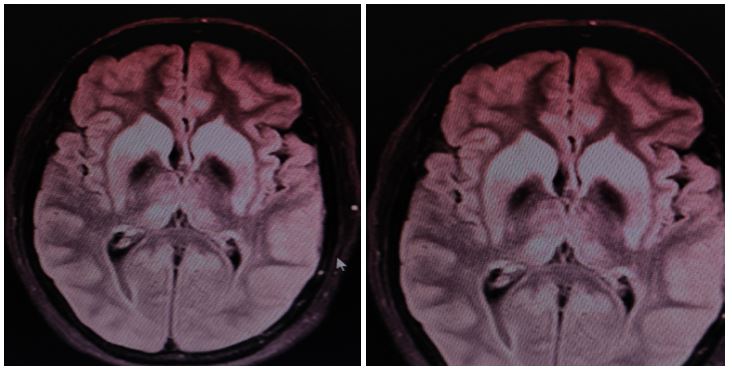
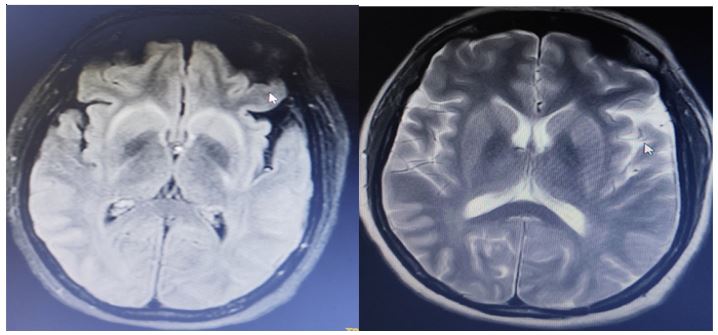
We report a case of a 61-year-old female presenting with fever for six days, followed by altered sensorium. MRI brain (contrast) revealed bilateral symmetrical edema of the cortical and deep grey matter, sparing the globus pallidus, suggestive of viral, metabolic, or toxic encephalitis. Extensive investigations, including meningoencephalitis panel, metabolic, autoimmune, and vasculitis workup, were negative. She was treated with IV methylprednisolone (1 g/day for five days), followed by a tapering steroid regimen, leading to clinical and radiological resolution. Follow-up MRI after five days of steroid therapy showed significant reduction in edema, supporting an immune-mediated etiology. This case highlights a rare, potentially para-infectious encephalopathy with complete reversibility following corticosteroid therapy.
Citation: Khosya S. A case of rapidly progressive encephalopathy with bilateral symmetrical deep grey matter involvement: A diagnostic dilemma. J Clin Images Med Case Rep. 2025; 6(3): 3526.
Introduction
Rapidly progressive encephalopathy presents a broad diagnostic challenge, with infectious, metabolic, toxic, autoimmune, and paraneoplastic causes being primary considerations. MRI findings of symmetrical basal ganglia and thalamic involvement often suggest viral or toxic encephalitis, yet similar patterns can be seen in autoimmune and para-infectious conditions. Early differentiation is critical for appropriate management [1].
We report a unique case of fever-associated encephalopathy with striking MRI abnormalities, negative infectious and autoimmune workup, and dramatic clinical and radiological improvement following immunosuppressive therapy.
Case presentation
History and examination
A 61-year-old female with no prior comorbidities presented with fever for six days, followed by altered sensorium.
GCS at admission: 10/15 (E3V2M5)
Neurological examination
No signs of meningeal irritation
Preserved motor responses (moving all four limbs to painful stimuli)
No seizures
No behavioral abnormalities
Investigations
MRI brain (Contrast study) (Day 1):
CSF analysis:
Protein: 68 mg/dL
Glucose: 62 mg/dL (RBS 138 mg/dL)
Cells: Within normal range
Meningoencephalitis panel: Negative (including HSV, JE, and arboviruses) [2].
Serum Ammonia, CBC, LFT, RFT: Normal
Autoimmune/vasculitis workup: Negative (NMDA-R, LGI1, ANA, ANCA, APLA)
Management and outcome
Given the absence of an identifiable infectious or metabolic cause and persistent encephalopathy, an immune-mediated mechanism was considered. The patient was started on IV methylprednisolone (1 g/day for five days), followed by oral steroid taper. Fever resolved within two days. Progressive neuro logical improvement over the next week. No seizures or behavioral disturbances during hospitalization. Follow-up MRI (Day 5 of steroid therapy)
Discussion
The combination of rapidly progressive encephalopathy, symmetrical basal ganglia-thalamic edema, and negative infectious/metabolic workup raised suspicion for a para-infectious or immune-mediated process.
Key differentials considered
1. Viral or toxic encephalopathy
CSF normal: No pleocytosis or viral markers.
No diffusion restriction: Makes toxic/metabolic causes unlikely [3].
2. Autoimmune/paraneoplastic encephalitis
Autoimmune panel negative, but antibody-negative autoimmune encephalitis is well documented [4].
3. Para-infectious immune-mediated encephalopathy
Preceding fever suggests post-viral inflammation. MRI changes match post-infectious demyelination patterns seen in ADEM-like syndromes [5].
Why this case is unique?
Steroid responsiveness and rapid MRI resolution confirm a treatable, inflammatory pathology. No relapse at three-month follow-up, suggesting self-limiting immune activation rather than chronic autoimmune encephalitis. Emphasizes early empirical corticosteroid therapy in unexplained encephalopathies [6].
Conclusion
This case highlights a steroid-responsive, non-infectious encephalopathy with bilateral symmetrical basal ganglia-thalamic involvement. The absence of a definitive infectious, metabolic, or autoimmune marker suggests an underrecognized para-infectious immune-mediated encephalopathy. Early corticosteroid therapy led to complete clinical and radiological recovery, emphasizing the importance of considering an inflammatory etiology in undiagnosed encephalopathies.
References
- Venkatesan A, et al. Autoimmune Encephalitis: Pathogenesis, Diagnosis, and Management. Neurology Clin. 2018; 36(2): 171- 186.
- Ellul MA, Solomon T. Acute encephalitis - diagnosis and management. Clin Med (Lond). 2018; 18(2): 155-159.
- Graus F, Titulaer MJ, Balu R, et al. A clinical approach to autoimmune encephalitis. Lancet Neurol. 2016; 15(4): 391-404.
- Dubey D, Pittock SJ, Kelly CR, et al. Autoimmune encephalitis epidemiology and response to immunotherapy. Neurology. 2018; 91(2): e160-e168.
- Hacohen Y, Rossor T, Mankad K, et al. Diagnostic algorithm for relapsing autoimmune encephalopathies in children. Neurology. 2017; 89(3): 236-248.
- Titulaer MJ, McCracken L, Gabilondo I, et al. Clinical spectrum of anti-NMDA receptor encephalitis. Brain. 2013; 136(Pt 6): 1905- 1917.