
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Supracarinal esotracheal fistula post surgery of a Type B aortic dissection associated with an aneurysm of a lusoria artery
Abdou Rabi R1
*; Sion A2
; Montagne F3
; Fournier C4
; Aulard Dorche W5
; Dubois C6
; Azzaoui R5
; Venissac N2
1University Hospital Center, Joseph Ravoahangy Andrianavalona, Antananarivo, Madagascar.
2Departement of Thoracic Surgery, University Hospital Center, Lille, France.
3Department of Thoracic Surgery, Valenciennes Hospital, Valenciennes, France.
4Pneumology Department, University hospital Center, Lille, France.
5Department of Vascular Surgery, University Hospital Center, Lille, France.
6Department of General and Digestive Surgery, Hospital University, Lille, France.
*Corresponding Author : Abdou Rabi R
University Hospital Center, Joseph Ravoahangy
Andrianavalona, Antananarivo, Madagascar.
Email: abdourabirichard@gmail.com
Received : Feb 14, 2025
Accepted : Mar 20, 2025
Published : Mar 27, 2025
Archived : www.jcimcr.org
Copyright : © Rabi RA (2025).
Abstract
Background: Acquired benign tracheoesophageal fistula is a rare pathology, leading to significant morbi-mortality. It represents a therapeutic challenge, requiring coordinated multidisciplinary management involving surgical resuscitators, interventional gastroenterologists and pulmonologists, anesthesiologists and thoracic surgeons. The diagnosis of Lusoria artery is often incidental. Due to development of an aneurysm, symptoms are secondary to compression of the aneurysm on adjacent structures such as the esophagus and the tracheobronchial tract. Moreover, the aneurysm can also become complicated.
Case report: We report our management of a tracheoesophageal fistula in a 64 years old man secondary of an acute necrosis of the esophagus, secondary due to a compressive hematoma of a dissection of the aneurysmal Lusoria artery. This man who presented dysphagia to solids and liquids and chest pain that had been evolving for 48 hours, was diagnosed on a CT scan with a dissection of the aortic isthmus, a dissection of the aneurysmal Lusoria artery and complicated by a fissure syndrome with a hematoma compressing the esophagus. After carotid-to-right subclavian bypass by cervicotomy first, followed by the placement of an aortoaortic tube by anterior thoracotomy, the post-operative course was marked by a tracheoesophageal fistula requiring an oesophagectomy and a tracheal covering by a muscle flap. Ventilatory support was done through 2 micro laryngeal tubes each positioned in a stem bronchus and a selective ventilation until the tracheal healing.
Keywords: Aberrant subclavian artery; Acute esophageal necrosis; Tracheoesophageal fistula; Conservative treatment; Selective intubation.
Citation: Rabi RA, Sion A, Montagne F, Fournier C, Dorche WA, et al. Supracarinal esotracheal fistula post surgery of a Type B aortic dissection associated with an aneurysm of a lusoria artery. J Clin Images Med Case Rep. 2025; 6(3): 3527.
Introduction
The aberrant right subclavian artery (ARSA) or Lusoria artery (LA) is the most common anomaly of the distribution of the aortic arch with an estimated incidence in the general population of 0.5 to 1.8% [1,2]. The LA course may lie either behind the esophagus in 80% of cases, between the esophagus and the trachea in 15% of cases, or even further forward, in front of the tracheobronchial tract in 5% of cases [3,4]. Tracheoesophageal fistula is defined as a pathological connection between the trachea and the esophagus, resulting in overflowing of oral and gastric secretions in the respiratory tract [5]. Its management is widely discussed with a lack of consensus among the different medical and surgical techniques not least because of the infrequency of this event. In our case, this tracheoesophageal fistula was secondary to an acute necrosis of the esophagus. The acute esophageal necrosis or “black esophageal necrosis” is a rare pathology, with an incidence of less than 0.2% in previous autopsy studies and from 0.01% to 0.2% in clinical trials [6]. Its pathogenesis is multifactorial, and ischemia is the most common etiology [7]. Our purpose is to report our management of a tracheoesophageal fistula due to a “black esophagus” caused by a compression of retro esophageal hematoma following a LA dissection.
Case report
A 64-year-old man presented to the emergency department with progressive dysphagia to solids and liquids and chest pain that had been evolving for 48 hours, following, according him, an osteopathy session. His medical history included an annuloectasiantic disease with an aortic insufficiency treated by the Bentall procedure with a mechanical valve replacement 10 years ago, a high blood pressure, a gastroesophageal reflux disease, an endoscopic polypectomy for intramucosal adenocarcinoma and smoking cessation with a tobacco consumption of 20 packs year.
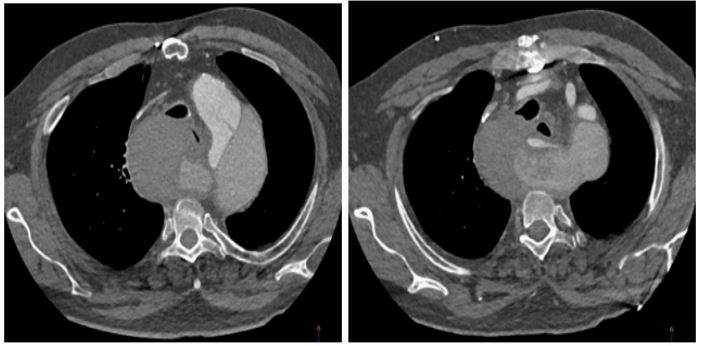
The patient was stable hemodynamically, without abnormalities at the physical examination. Morphological findings, including a chest X-ray, revealed an enlarged mediastinum. An emergency thoracic CT scan revealed a dissection of the aortic isthmus, measured at 62 mm in superior diameter, and a dissection of the aneurysmal LA, measured at 78 mm in diameter complicated by a fissure syndrome with a hematoma compressing the esophagus. On the 2011 CT scan, the LA was described. The right vertebral artery arose from the true channel of the subclavian (Figure 1) (See appendix 1 for a video of CT scan). The Bentall surgical mounting was seamless.
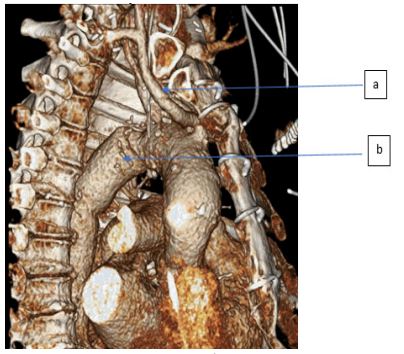
The patient underwent an emergency surgery (Figure 2) with an extracorporeal life support (ECLS). Firstly, a carotid bypass to the right subclavian was perfomed by cervicotomy. Then the aneurysm was excluded by the placement of an aortoaortic tube by anterior thoracotomy with aortic clamping between the common carotid artery and the left subclavian artery.
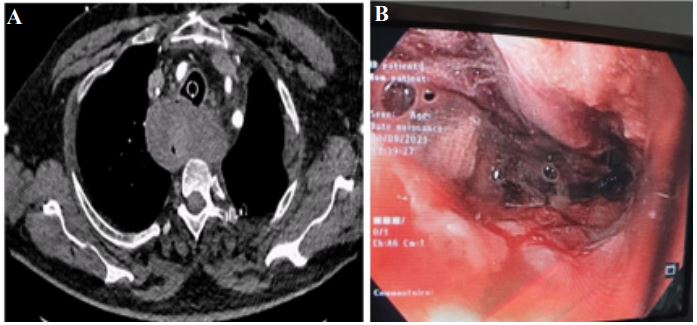
Surgical follow-ups were straightforward up to day 2. The patient was at day 1 extubated and vasopressor amines weaned. At day two, the patient became more severe, presenting with dyspnea and bloody, dry sputum, before finally presenting with respiratory distress requiring intubation and mechanical ventilation. On the chest CT scan was identified a retrotracheal hematoma without abnormalities of the vascular surgical assembly. The nature of the sputum was such that an eso-gastroduodenal fiboscopy was performed, which revealed a black esophagus with necrotic oesophageal mucosa over 5 cm to 20 cm from the dental arches (Figure 3).
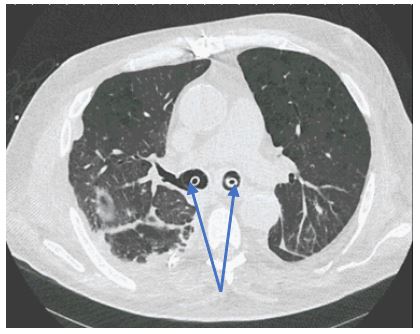
After a collegial multidisciplinary discussion with surgical resuscitators, interventional gastroenterologists and digestive surgeons, the patient had received first a conservative medical treatment including proton pump inhibitors and a close medical monitoring. At day 6, given the persistence of sepsis and the occurrence of ARDS, a tracheotomy was indicated for a prolonged mechanical ventilation. Before this tracheotomy a bronchial fibroscopy revealed a supracarian fistula located 5 cm under the vocal cords with a doubt on the communication with the esophagus. So, respiratory support required to by-pass the fistula and it was done through 2 micro laryngeal tubes (MLT), each positioned in a stem bronchus, by the tracheotomy and a selective ventilation (Figure 4) (See appendix 2 for a video of CT scan). Meanwhile, by a right thoracotomy, an esophagectomy was performed, with a cervical esophagostomy and a feeding jejunostomy was inserted also. Healing management of the tracheal fistula required to cover the fistula with an intercostal muscle flap interposed in front of the tracheal fistula.
(B) Dissection of the sub-artery right retroesophageal aneurysm.
The patient will then remain under an exclusive mechanical ventilation, sedated and curarized, until the complete healing of the tracheal plasty, which will occur at post operative day 30. Then the 2 MLT were replaced by a single lumen tracheotomy cannula. Between postoperative day 6 and 30, the patient has presented some complications as:
• Ventilatory difficulties resulting in permissive hypercapnia.
• Recurrent atrial fibrillation requiring electrical cardioversion then followed by a right ventricular failure treated by inhaled NITRIC OXIDE and SILDENAFIL CITRATE.
• An acute multi-factorial renal failure due to the surgery, right ventricular dysfunction, some cumulative drugs’ nephrotoxicity, and the sepsis. This required temporary dialysis.
• A mediastinitis with retrotracheal collection at post operative day 14 requiring surgical debridement and a targeted antibiotitherapy for E. coli Tazocillin resistant, and E. aerogenes and E. faecium.
• This therapy was incremented by MEROPENEM and TEICOPLAMINE, then switched by CEFEPIM and DAPTOMYCIN in front of a severe toxiderma potentially incriminating both molecules and PANTOPRAZOLE.
• Then a liver cytolysis followed by cholestasis, without evidence of a biliary obstruction and maybe due to a hypoxic etiology.
For long-term, after recovery from his intensive care neuropathy, the patient could be weaned from his tracheotomy 7 months later. The last bronchial fibroscopy revealed no persistent fistula. There was also a good mobility of the pharynx and vocal cords. One year later, a surgery to restore digestive continuity through gastroplasty was performed, followed by multiples endoscopic esophageal dilatations and esophageal prothesis.
Discussion
The first known anatomical description of the ARSA was done by Hunauld in 1735. Bayford, in 1794, described the dysphagia lusoria [1], due to the ARSA. Most ARSA symptoms are related to development of aneurysmal diseases located at the origin of the artery. This aneurysm occurs in nearly 60% of ARSA cases [8]. The diagnosis of LA is often incidental, as only 5% of patients with this variation will develop symptoms [3,9]. Symptoms are due to the compression of the aneuvrysm on adjacent structures as the esophagus and the tracheobronchial tract, leading to dysphagia, dyspnoea, chronic cough, stridor by compression of the recurrent laryngeal nerve and chest pain. Aneurysm also becomes complicated, leading rupture, dissection and, rarely, distal embolization [10]. The ARSA may be associated with other vascular variations such as bicarotic trunk (19.2%), Kommerell diverticulum (14.9%), artery aneurysm itself (12.8%) and a right aortic arch (9.2%) [1,3].
Kieffer in 1994 proposed a classification based on the clinical manifestations of ARSA:
• Type 1 implies dysphagia caused by a nonaneurysmal ARSA
• Type 2 includes ischemic symptoms caused by occlusive disease of a nonaneurysmal ARSA
• Type 3 is an aneurysm with or without symptoms of ARSA
• Type 4 includes ARSA arising from a diseased, usually aneurysmal, thoracic aorta with or without ARSA [8].
Recently, Yang et al, [9] in a review on aberrant subclavian arteries, updated this classification with 5th group including iatrogenic injuries and by dividing type 4 into two subgroups:
• Type 4a which is an ARSA from aneurysmal thoracic aorta.
• Type 4b which is an aortic dissection arising from an ARSA.
Rupture is the most severe and urgent complication of the ARSA aneurysm with a mortality rate of 50% in the case of an acute rupture. It’s rate ranges from 6% to 19%. Esophageal fistula secondary to ARSA is also rare, but is associated to high mortality due to a late diagnosis. Fistula often results from the posterior compression by the ARSA aneurysm, leading to upper gastrointestinal bleeding. Other rupture causes include trauma from nasogastric or endotracheal tubes or endovascular catheters [9].
Our post-operative follow-up were marked by a retro tracheoesophageal hematoma compressing the esophagus, leading to an ischemia of the esophageal wall - black esophagus- at FOGD, followed by a tracheoesophageal fistula.
Acute necrotizing esophagitis (ANO) also known as acute esophageal necrosis, Black esophagus or Gurvits syndrome is a rare but potentially devastating pathology characterized in endoscopy by necrosis of the esophageal mucosa causing ulcerated and necrotic blackish circumferential lesions of the mucosa. ANO was first described by Goldenberg and al. in 1990, its prevalence ranges from 0.001% to 0.28% depending on the series [11]. It mainly affects older men, with a median age at 75 years, and a sex ratio of 3/1. The most common etiology is low-flow ischemia secondary to cardiac dysfunction or septic shock. Other causes of ANO are gastric transit obstruction with massive gastroesophageal reflux, hypothermia, and hypersensitivity to antibiotics such as Tetracyclin and Clindamycin inducing oesophageal injury and producing direct toxic effects in the oesophageal mucosa [12]. Comorbidities such as diabetes, ethylism, coronary artery disease, high blood pressure, and chronical kidney failure can also promote ANO. Most authors recommend a conservative but aggressive therapeutic approach that includes correction of glycemic disorders, total parenteral nutrition, intravenous high-dose proton pump inhibitors and administration of sucralfate, adequate intravenous hydration, broad-spectrum antibiotics if germs have been identified or suspected esophageal perforation [6,12-14]. The most common mid-term complication of ANO is tracheoesophageal fistula in 30% of cases with a mortality rate of 29.9% and the most long-term complication is esophageal stenosis, with a rate of 70% in a literature review [7].
We report a Stanford B dissection associated with an ARSA aneurysmal, which is a rare entity without established standard management.
Different surgical techniques such as open surgery or, endovascular and hybrid techniques combining open surgery and endovascular have not yet reached international consensus. Verzini and al [8] reported a hybrid approach by «Bilateral carotid-subclavian bypass and a thoracic endovascular aortic repair with ARSA and left subclavian ostia coverage» in 71,5% of scheduled surgery, but not in emergency condition. Using these hybrid techniques, the plug is positioned in the arterial segment which overlays the esophagus. Consequently, dysphagia could be persistent due to the plug compression. Furthermore, the close proximity carries the potential risk for a fatal subclavian esophageal fistula [9,10].
In our case, our vascular colleagues decided to perform:
• Fisrt, a carotid bypass under the ARSA by cervicotomy.
• Then, under an ECLS, the exclusion of the aortic aneurysm by an aorto-aortic tube with an aortic clamping between the left common carotid and the left subclavian artery by an anterior thoracotomy.
• This approach was indicated for our colleagues, taking account previous bad endovascular surgery experience in ARSA, the potential instability of the vascular assembly, and the untreated dysphagia consequence and the posterior mediastinitis.
Post-operative course of our patient was followed-up by a retro tracheoesophageal hematoma compressing the esophagus, leading to an ischemia of the esophageal wall with the diagnosis of a black esophagus at FOGD, then followed by a tracheoesophageal fistula. Several contributing factors may be found in our case, with intrinsic patient’s factors high blood pressure, past smoking consumption, gastro-reflux esophageal; and also, extrinsic factors which are ECLS with its disseminated inflammatory reaction leading to endothelial tissue damages and vasomotor dysfunction as well as excessive fibroproliferative response [15], and compression of the esophagus by the hematoma secondary to the dissection of the retro-esophageal right subclavian artery. This esophageal necrosis by extrinsic compression of the aortic dissection, the compressive hematoma or the esophageal ischemia secondary to extended thrombosis in false light of aortic dissection, thus obstructing the blood flow to the intercostal arteries and the esophagus has been described in literature [5,13,16].
Airways protection against gastric contents is an emergency and must be quickly anticipated if a tracheoesophageal fistula occurred. Inhalation pneumonia by digestive fluids will lead to major complications such as septic shock and mediastinitis. Airways protection can be achieved if the fistula is high by positioning the endotracheal tube balloon under the fistula with a tracheostomy downstream of the fistula. Nasogastric or orogastric tubes should be removed to prevent pressure-related esophageal necrosis spreading. This is particularly true for intubated patients. They should be placed in a half-sitting position at 45°, high oral aspirations should be frequent, and a gastrostomy may be considered. Efficient enteral nutrition via a jejunostomy should be performed also.
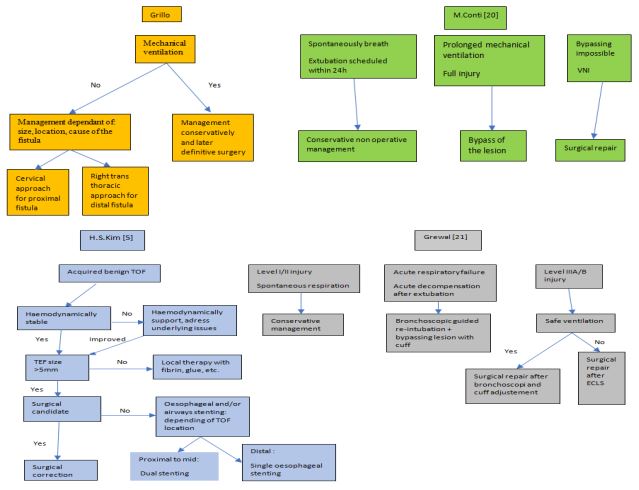
Grillo in 2004 described an individual management of benign fistula not related to ventilation depending on their cause, size, location, and degree of surrounding pathology. Cervical and cervicothoracic approaches, less frequently right transthoracic are used depending on the level of the fistula. Only a supracarinal fistula requires a thoracotomy.
Massimo Conti and al [17] recommended conservative nonoperative management of post-intubation tracheobronchial rupture as the best approach in patients who breathe spontaneously, or when extubation is scheduled within 24 hours from the time of diagnosis, and for patients who require prolonged mechanical ventilation to treat their underlying respiratory condition. Surgical repair should be reserved for patients on non-invasive ventilation and if bypassing the lesion is technically impossible. The mortality rate is higher for patients surgically managed compared to those who received a conservative treatment, of 23% and 16%, respectively; p 0.475. If a surgery is required, the first step is to determine the appropriate intraoperative anesthetic and ventilation management to maintain oxygenation. Selective intraoperative pulmonary intubation with selective endotracheal tube placed by bronchoscopy, is chosen to circumvent the tracheal lesion. When the lesion concerned the distal third of the trachea, or even the first centimeter of a stem bronchus, selective bilateral bronchial intubation with high volume/low pressure balloon is indicated.
There is no international consensus on the management of tracheal lesions, and Cardillo et al. [18] proposed a classification of airway lacerations according to their morphology to guide their management. Thus, an incomplete rupture of the muscular wall (grade I, II) or a simple complete rupture of the wall (grade IIIA) can be treated by a conservatrive non-operative approach. The surgical approach is necessary in case of complete laceration associated with concomitant esophageal lesion or mediastinitis (grade IIIB).
A post-intubation tracheo-bronchial lesion management algorithm has been established by Conti and al. in 2005, and improved by Boutros et al. in 2022. The first decision criterion is the need for mechanical ventilation and the second criterion consisted of a possibility of by-passing the lesion to facilitate the choice between conservative management on the one hand or surgical management on the other [19,20]. Grewal et al [21] in 2019 described an algorithm approach for the contemporary treatment of tracheobronchial injuries according to morphological tracheal injury and the presence of an acute respiratory failure. Patients with level I/II injury with spontaneous respiration are treated with conservative management, and those with acute respiratory failure or acute decompensation after extubation, may require bronchoscopic guided re-inubation to place the endotracheal tube cuff beyond the injury site. Patients with level IIIA/B injury require surgical repair. To assist ventilation, a mechanical ventilation can be performed after a bronchoscopic cuff adjustment to by-pass the tracheal injury, or in case of ventilation failure as a bridge to recovery and/or definitive surgery an extracorporeal membrane may be necessary.
The endoscopic tracheal stenting is an alternative to endotracheal tubes to exclude the tracheal fistula. This has been described in the review of Kim HS et al. [5] as the most viable and best studied intervention with the best quality of life for patients with malignant tracheoesophageal fistula requiring palliative intervention, or benign tracheoesophageal fistula that require stenting before a radical surgery. This tracheal stenting is indicated for proximal to mid fistulas with the use of silicone stents, straight or Y, and self-expanding metal stents. All those devices have advantages and disadvantages leaving the choice to the bronchoscopist.
An esophageal prosthesis or a double tracheo-esophageal stenting allowing a structural support on both sides of the fistula were also described. The dual-stenting approach provides a protective strategy against airway compression by oesophageal stents and their migration into the airways. To further prevent airway compression, airway stents are always placed first, followed by oesophageal stents [5]. Herth et al. [22], studied the efficacy of dual stenting versus single stenting. Out of 112 patients, 65(58%) received a single airway stent, 37(33%) received a single esophageal stent and 10(9%) received dual stents. A better survival was observed in dual stents condition (245 days) versus tracheal stent (182 days).
Hyun S. Kim [5] in his review purposed an algorithm of the tracheo-oesophageal fistula management. Benign fistula is more amenable to definitive surgical intervention when the size of the fistula is >5 mm, associated with a hemodynamically stable patient. However, if the patient requires medical optimization and is not a surgical candidate, an esophageal endoprosthesis in the distal fistulas or double-stented airways can be performed in the proximal to mid.
For our patient, we performed the fistula exclusion using two 6 mm endotracheal MLT in the stem bronchi as described above through the tracheotomy. This was indicated by the distal location of the fistula in pre-carenary, and the long-term mechanical ventilation needed to bypass positive pressure exposure. This management requires a well close coordinated, and rapid collaboration between anesthetists, surgical resuscitators, interventionist pulmonologists and thoracic surgeons. Due to the esophageal necrosis, a radical esophageactomy with cervical esophagostomy and feeding jejunostomy were indicated and carried out, for the primary prevention of mediastinitis, followed by the tracheal fistula coverage using an inter costal muscle flap.
Conclusion
Tracheoesophageal fistula is an uncommon pathology difficult to cure. Our case report reminds us that a mediastinum hematoma can be grafted from a serious evolution and is a real challenge for medical actors. More often, benign tracheoesophageal fistula is more amenable to definitive surgical intervention due to the transient nature of the injury and better nutritional status, and the choice between conservative approach, definitive surgery, endoscopic tracheal stenting, oesophagus stenting or dual stenting will depend on combination of patient’s condition, the location, morphological tracheal injury and the presence of an acute respiratory failure. Airways protection is an emergency condition. So, bypassing the tracheoesophageal fistula must be done quickly. The use of MLT placed beyond the injury site, is an interesting option for patients who require prolonged mechanical ventilation to treat their underlying respiratory condition. Moreover, this kind of rare disease highlight the importance of a coordinated multidisciplinary team management involving surgical resuscitators, interventional gastroenterologists and pulmonologists, as well as anesthesiologists and thoracic surgeons.
References
- Carles D, Pelluard F, André G, Nocart N, Sauvestre F. Aberrant right subclavian artery (arteria lusoria) and the risk for trisomy 21. Retrospective study of 11,479 fetopathological examinations. J Gynécologie Obstétrique Biol Reprod. 2014; 43(9): 698‑703.
- Stone WM, Ricotta JJ, Fowl RJ, Garg N, Bower TC, Money SR. Contemporary management of aberrant right subclavian arteries. Ann Chir Vasc. 2011; 25(4): 545-51.
- Chowdhury Y, A. Shaikh S, Salman A, D. Marmur J, M. McFarlane Isabel. Aberrant Right Subclavian Artery and Stanford Type B Aortic Dissection. Am J Med Case Rep. 2020; 8(8): 247‑9.
- Fanelli U, Iannarella R, Meoli A, Gismondi P, Cella S, Vincenzi F, et al. An Unusual Dysphagia for Solids in a 17-Year-Old Girl Due To a Lusoria Artery: A Case Report and Review of the Literature. Int J Environ Res Public Health. 2020; 17(10): 3581.
- Hyun S. Kim, Danai Khemasuwan, Javier Diaz-Mendoza and Atul C. Mehta. Management of tracheo-oesophageal fistula in adults. Eur Respir Rev. 2020; 29: 200094.
- Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: a rare syndrome. J Gastroenterol. 2007; 42(1): 29‑38.
- Schizas D, Theochari NA, Mylonas KS, Kanavidis P, Spartalis E, Triantafyllou S, et al. Acute esophageal necrosis: A systematic review and pooled analysis. World J Gastrointest Surg. 2020; 12(3): 104-15.
- Verzini F, Isernia G, Simonte G, De Rango P, Cao P, Castelli P, et al. Results of aberrant right subclavian artery aneurysm repair. J Vasc Surg. 2015; 62(2): 343-50.
- Yang C, Shu C, Li M, Li Q, Kopp R. Aberrant Subclavian Artery Pathologies and Kommerell’s Diverticulum: A Review and Analysis of Published Endovascular/Hybrid Treatment Options. J Endovasc Ther. 2012; 19(3): 373‑82.
- Jalaie H, Grommes J, Sailer A, Greiner A, Binnebösel M, Kalder J, et al. Treatment of Symptomatic Aberrant Subclavian Arteries. Eur J Vasc Endovasc Surg. 2014; 48(5): 521-6.
- Dias E, Antunes JS, Macedo G. Diagnosis and management of acute esophageal necrosis. Annals of Gastroenterology. 2019; 32: 529-540.
- Petersen KU, Jaspersen D. Medication induced oesophageal disorders.Expert Opin. Drug Saf. 2003; 2(5): 495-507.
- Gurvits GE, Cherian K, Shami MN, Korabathina R, El-Nader EMA, Rayapudi K, et al. Black Esophagus: New Insights and Multicenter International Experience in 2014. Dig Dis Sci. 2015; 60(2): 444-53.
- van de Wal-Visscher E, Nieuwenhuijsen GAP, van Sambeek MRHM, Haanschoten M, Botman KJ, de Hingh IHJT. Type B Aortic Dissection Resulting in Acute Esophageal Necrosis. Ann Vasc Surg. 2011; 25(6): 837.e1-837.e3.
- Lanquetot H, Charrière JM, Soubiron L, Chauvet S, Mandon N, Vilain O, et al. Vasoreactivity changes during extracorporeal circulation: effects of halogenated agents. Ann Fr Anesth Réanimation. 2012; 31: S34‑9.
- Conrad L, Pinheiro M, Mais L. Acute oesophageal necrosis: A rare complication. Rev Médecine Interne. 2022; S0248866321011164.
- Conti M, Pougeoise M, Wurtz A, Porte H, Fourrier F, Ramon P, et al. Management of Postintubation Tracheobronchial Ruptures. Chest. Août. 2006; 130(2): 412-8.
- Cardillo G, Carbone L, Carleo F, Batzella S, Jacono RD, Lucantoni G, Galluccio G. Tracheal lacerations after endotracheal intubation: a proposed morphological classification to guide non-surgical treatment. European Journal of Cardio-thoracic Surgery. 2010; 37: 581-587.
- Boutros J, Marquette C-H, Ichai C, et al. Multidisciplinary management of tracheobronchial injury. Eur Respir Rev. 2022; 31: 210126.
- Conti M, Fournier C, Hysi I, Ramon P.P, Wurtz A. Conservative management of post intubation tracheal membrane ruptures. Intensive Care Med. 2010; 36: 1622-1623.
- Grewal HS, Dangayach NS, Ahmad U, Ghosh S, Gildea T, Mehta AC. Treatment of Tracheobronchial Injuries. Chest. 2019; 155(3): 595-604.
- Herth FJ, Peter S, Baty F, et al. Combined airway and oesophageal stenting in malignant airway oesophageal fistulas: a prospective study. Eur Respir J. 2010; 36: 1370–1374.