
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Novel fact for the therapeutics of hepatic metastases from gastric cancer
Amel Azouzi1 ; Faiza Taib1 ; Sabeha Belhouas1 ; Abdellah Boudiaf1 ; Salim Belkherchi2 ; Salah Berkane1*
1University Benyoucef Benkheda, Faculty of Medicine of Algiers, Algiers, Algeria.
2University and Teaching Hospital of Bejaia, University Abderahmane Mira of Bejaia, Faculty of Medicine of Bejaia, Algeria.
*Corresponding Author : Salah Berkane
University Benyoucef Benkheda, Faculty of Medicine
of Algiers, Algiers, Algeria.
Email: salahberkane07@yahoo.fr
Received : Feb 24, 2025
Accepted : Mar 21, 2025
Published : Mar 28, 2025
Archived : www.jcimcr.org
Copyright : © Berkane S (2025).
Abstract
Gastric cancer is the fifth most common malignant tumor location and the fourth leading cause of cancer-related death worldwide [1]. The occurrence of hepatic metastases in gastric cancer makes the prognosis very poor in the short term and the average survival from the time of diagnosis is 3 months. The only curative treatment is radical resection of the hepatic metastases, but this eventuality is rare [2]. The metastasis occur during two different periods: Either in a synchronous situation (before any treatment of gastric cancer or occurring within 6 months after gastrectomy) or in a metachronous situation (occurring 6 months after gastrectomy). At the initial time of diagnosis, approximately 4 to 14% of patients with gastric cancer have synchronous liver metastases, while approximately 37% of patients with gastric cancer will develop metachronous liver metastases after gastrectomy [3]. In this article, we report the case of a patient treated with curative intent for a single metachronous hepatic metastasis and still alive more than 12 years.
Keywords: Radical Surgery; Hepatectomy; Neoadjuvant Chemotherapy;
Citation: Azouzi A, Taib F, Belhouas S, Boudiaf A, Belkherchi S, Berkane S. Novel fact for the therapeutics of hepatic metastases from gastric cancer. J Clin Images Med Case Rep. 2025; 6(3): 3529.
Case report
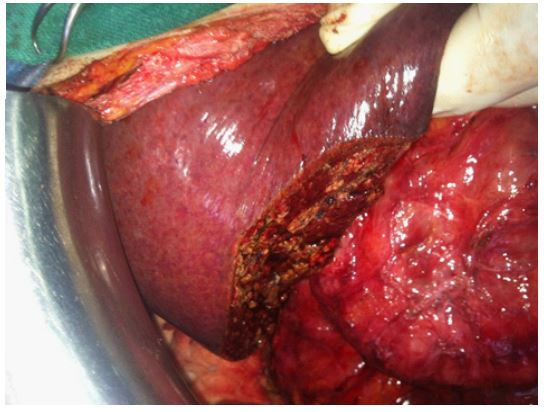
This is a 73-year-old patient with a history of non-insulindependent diabetes hospitalized in our department for the management of gastric adenocarcinoma diagnosed following the onset of atypical and mild epighastralgia. The clinical examination on admission is normal. The preoperative assessment (an esophagogastroduodenal fiborscopy plus biopsy, à CT scan and biological tests) showed a tumor of the angulus without locoregional or distant extension classified. The tumor was classified pT4a N0 M0. The endoscopic biopsy was in favor of a poorly differentiated adenocarcinoma with a negative HER2 status. On this finding, surgery was proposed to the patient. Intraoperative exploration showed the existence of a tumor of 60 mm in large diameter and 27 mm in thickness, of angular site with infiltrated serosa and without locoregional or distant extension. A total gastrectomy was performed with a type D2 lymphadenectomy according to Maruyama. The follow-up was punctuated by a minor complication such as wall sepsis which required local care. At the same time, the patient’s diabetes disappeared and the hypoglycemic treatment was stopped. Macroscopic and histological examination of the surgical specimen showed an ulceroinfiltrating tumor of 60 mm in diameter and a poorly differentiated adenocarcinoma affecting the serosa. The 8 lymph nodes recovered by curettage were healthy and the peritoneal cytology was benign. The patient received 3 courses of adjuvant systemic chemotherapy based on ECF (Epirubicine + Cisplatine + 5flurouracile) without complications. At the 10th postoperative month, a liver metastasis located in segments VI and VII of 90 x 63 mm was revealed on CT scan associated with 3 hypertrophied and suspicious adenopathies in the lateroaortic region. The carbohydrate antigen 19.9 (CA 19.9) and the carcinoembryonic antigen (CEA) had the respective values of 16.43 IU/ml (Normal) and 127 ng/ml (52x normal). After discussion with the medical oncologists, it was decided to perform neoadjuvant chemotherapy with 6 courses of LV5FU2CIS (Lederfoline + 5Flurouracile + Cisplatine) and to operate on the patient at the end in the event of an objective response (reduction in size and disappearance of lymph nodes). At the end of this neoadjuvant therapy, the tumor diameter decreased to 36mm and the images of suspicious lymph node disappeared. No other lesions appeared. The CEA dropped to 12.47 ng/ml (2x Normal) and the CA 19.9 was measured at 22.99 IU/ml (Normal). Given the good general condition of the patient, the tumor response and the possibility of a minor hepatic resection, surgery to resect this metastasis was chosen. It should be noted that the patient’s diabetes disappeared after the gastrectomy. This procedure was performed 15 months after the end of neoadjuvant systemic chemotherapy. Intraoperative exploration confirmed the existence of a 30 mm metastasis, hard and whitish, located at the level of segment VI without any other associated lesion, in particular no retroparitoneal lymph node and absence of peritoneal carcinomatosis nodule. Intraoperative ultrasound did not show other suspicious liver foci. A metastasectomy was performed without clamping. This procedure took place with a total bleeding of 500 and no transfusion was necessary. The postoperative course was simple. Histological examination of the surgical specimen showed the existence of a partly necrotic liver metastasis and with healthy section slices. An additional 6 courses of LV5FU2CIS were performed postoperatively. years The patient is alive without recurrence at more than 12 years after the hepatectomy and 13 years after gastrectomy with a good general condition, without intestinal disorders and a normal diet. His blood sugar is normal. He presented with postgastrectomy gallstones complicated by an episode of cholangitis which was treated medically. He is awaiting cholecystectomy for his gallstones.He presented with posg gallstones.

Discussion
Hepatic metastasis is the most common hematogenous site of gastric cancer. MZ Qiu et al [4] reported from SEER (Surveillance, Epidemiology, and End Results) data that the frequency of metastases at diagnosis (synchronous metastases) was 41% (7,792 of 19,022 patients) and the majority of these hematogenous metastases were hepatic (3,218 patients). Among gastric cancers with synchronous hepatic metastases, 70% (2,247 of 3,218 patients) of patients had isolated hepatic metastases and the rest of patients had at least one other metastatic focus. Since the early 1990s, some retrospective studies and small series have shown that radical liver resection surgery improved the prognosis [5]. Thus, 5-year survival ranged from 9 to 42% with a median duration of 12 to 41 months after radical hepatectomy for liver metastases from gastric cancer. Di Long et al [6] reported their study in 2016 on the surgical management of liver metastases of gastric origin. This study totaled 39 studies that included a median number of 21 liver resections (10- 64). Liver resection was associated with a 30-day morbidity of 24% and a 30-day mortality of 0% (0%-30%). Overall survival at 1 year, 3 years and 5 years was 68%, 31% and 27%, respectively. For these authors, Asian studies reported a higher survival than that reported by Western studies with (73% vs 59% for 1-year survival, 34% vs 25% for 3-year survival and 27% vs 17% for 5-year survival. Furthermore, when the authors compare palliative treatment with resection, they show a significant reduction in gastric cancer mortality at 1 year (risk ratio [RR] 0.47, P< 0.001) and at 2 years (RR 0.70, P< 0.001). C. Monroy et al reported on their meta-analysis an overall survival at 1 year, 3 years and 5 years of 69.79%, 34.79% and 24.68% while recurrence-free survival at the same dates is 41.39%, 23.23%, and 20.18% [7]. In this meta-analysis, the authors identified the following factors as good prognostic factors linked to better survival: the occurrence of metachronous metastasis, good differentiation of the primary tumor, a small metastasis, minor lymph node involvement, R0 resection, and a solitary unilobar situation. When the metastasis is single and small, recurrence-free survival is longer. Corina-Elena Minciuna et al [8] conducted a study in 28 patients with gastric cancer associated with synchronous liver metastases, 16 of whom underwent gastrectomy associated with liver resection of these liver metastases (GR group), while 12 underwent isolated gastrectomy without liver resection (SR group). The median survival of the entire series (OS) was 18.81 months with 1-, 3- and 5-year survival of 71.4%, 17.9% and 14.3%, respectively. The overall survival at 1, 3 and 5 years for the GR group was 75%, 31.3% and 25% significantly higher than that of the SR group which was 66.7%, 0% and 0% (p = 0.004). Multivariate analysis of the cohort showed that only hepatic resection was a good prognostic factor (HR = 3.954, 95% CI: 1.542–10.139; p = 0.004). Their conclusion was that in this Western cohort, synchronous resection of gastric cancer metastases significantly improves overall survival compared to pallia-tive gastrectomy. In addition to radical hepatic resection, neoadjuvant or adjuvant systemic chemotherapy seems to provide a plus in association with hepatic resection [9,10]. The goals of this neoadjuvant therapy are to make metastatic disease resectable or to reinforce the action of the first radical resection [11]. Our observation illustrates this fact well in that the tumor diameter was divided by 3 and the lateroaortic lymph nodes disappeared after neoadjuvant chemotherapy. There is the illustration, even if it is a single case, that chemotherapy can have an action on both hepatic and lymph nodes metastasis. This is an avenue to explore
Conclusion
Our observation clearly illustrates that the radical approach to a hepatic localization of a gastric adenocarcinoma involves radical excision surgery, which is the basis of management. At the same time, the association with neoadjuvant and/or adjuvant systemic chemotherapy helps to consolidate long-term results.
References
- Li B, Liu HY, Guo SH, et al. Detection of microsatellite instability in gastric cancer and dysplasia tissues. Int J Clin Exp Med. 2015; 8: 21442-21447.
- Negoi I, Runcanu A, Paun S, Negoi RI, Mircea Beuran M. Resection of Large Metachronous Liver Metastasis with Gastric Origin : Case Report and Review of the Literature. 8(10): 814. DOI 10.7759/cureus.814.
- Luo Z, Rong Z. Huang C. Surgery Strategies for Gastric Cancer With Liver Metastasis Frontiers in Oncology. 2019; 9:1353. www.frontiersin.org.
- Qui MZ, Shi SM, Che ZH, Yu H, Sheng H, Jin Y,et al. Frequency and clinicopathological features of metastasis to liver, lung, bone, and brain from gastric cancer: A SEER-based study. Cancer Med 2018; 7: 3662-72.
- Okano K, Maeba T, Ishimura K, Karasawa Y, Goda F, et al. Hepatic Resectio n for Metastatic Tumors From Gastric Cancer. Ann Surg; 235: 9186-91
- Long Di, Yu PC, Huang W, Luo YL, Zhang S. Systematic review of partial hepatic resection to treat hepatic metastases in patients with gastric cancer. 2016; 95: 44.
- Monroy DC, Ibañez-Pinilla M, Sabogal JC, Rey Chaves C, IsazaRestrepo A, et al. Outcomes of Hepatectomy in Gastric, Cancer Liver Metastasis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023 ; 12 : 704. https://doi.org/10.3390/ jcm12020704.
- Minciuna CE, Tudor S, Micu S, Diaconescu A, Alexandrescu A, S T, et al. Safety and Efficacy of Simultaneous Resection of Gastric Carcinoma and Synchronous Liver Metastasis-A Western Center Experience. 2022 ; 58 : 1802. https://doi.org/ 10.3390/medicina58121802.
- Becker K, Mueller JD, Schulmacher C, Ott K, Fink U, et al. Histomorphology and Grading of Regression in Gastric Carcinoma Treated with Neoadjuvant Chemotherapy Cancer. 2003; 98: 1521-30.
- Glimelius B, Ekstrom K, Hoffman K, et al. Randomized comparison between chemotherapy plus best supportive care with best supportive care in advanced gastric cancer. 1997; 8: 163-8.
- Miceli R, Tomasello G, Bregni G, Di Bartolomeo M, Pietrantonio F. Adjuvant chemotherapy for gastric cancer : Current evidence and future challenges. World J Gastroenterol 2014; 20(16): 4516-4525.