
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 6
Giant molluscum contagiosum in an immunocompetent patient
Soukayna Kabbou SK*; Ouiam Eljouari OE; Hardouzi Hala HH; Salim Gallouj SG
Dermatology Department, University Hospital Center Mohammed VI, Tangier 40000, Morocco.
*Corresponding Author : Soukayna Kabbou SK
Dermatology Department, University Hospital
Center Mohammed VI, Tangier 40000, Morocco.
Tel: 00212615820850;
Email: soukayna.kabbou@usmba.ac.ma
Received : Mar 01, 2025
Accepted : Mar 21, 2025
Published : Mar 28, 2025
Archived : www.jcimcr.org
Copyright : © Kabbou SKS (2025).
Keywords: Giant; Molluscum contagiosum; Immunocompetent.
Citation: Kabbou SKS, Eljouari OEO, Hala HHH, Gallouj SGS. Giant molluscum contagiosum in an immunocompetent patient. J Clin Images Med Case Rep. 2025; 6(3): 3530.
Description
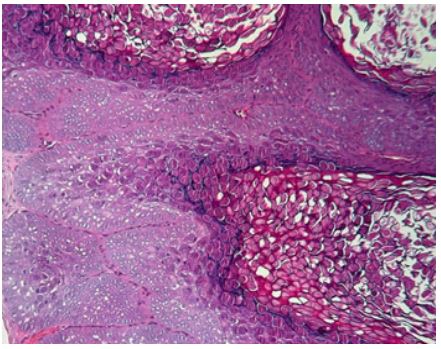
A 20-year-old male presented with a solitary erythematous nodule that had gradually increased in size over the past four months. The lesion was repeatedly traumatized by scratching, leading to occasional episodes of bleeding, raising the possibility of pyogenic granuloma as a diagnosis. On examination, a large, firm, skin-colored to pink nodule measuring 12 mm was located on the left temporal region (Figure 1a ). The lesion featured peripheral erosion, crusting and central umbilication. Dermoscopy objectives yellow amorphous structures with peripheral radially arranged fine linear vessels (Figure 1b). The clinical presentation strongly suggested a diagnosis of molluscum contagiosum (MC). The lesion was extirpated with electro-dessication of the base. The diagnosis of giant MC was confirmed by the histological examination, which showed large keratinocytes with distinctive eosinophilic Henderson-Patterson inclusion bodies. HIV serology was negative. MC is a benign cutaneous infection caused by a double-stranded DNA virus of the Poxviridae family. It is typically transmitted through direct contact with an infected individual or via contaminated surfaces [1]. The typical appearance of MC is papules of flesh color with a central umbilication measuring 3-5 mm in size. However, atypical lesions, referred to as Giant Molluscum Contagiosum, can grow to considerably larger sizes, ranging from 10-15 mm [2]. This variant is rarely seen in immunocompetent individuals, such as our patient, and is more frequently associated with immunosuppressive conditions, including AIDS, leukemia, or those receiving immunosuppressive therapy [3]. Although MC is mainly diagnosed clinically, in cases with atypical presentation, histopathological examination or PCR may be required to distinguish it from other conditions such as foreign body granuloma, keratoacanthoma [4] , or botryomycoma, as observed in the present case. Treatment options include curettage, cryotherapy, and topical agents like imiquimod 5% cream, salicylic acid 10% gel, or retinoic acid 0.5% cream. Furthermore, cauterization may be used with caustic agents like phenol or trichloroacetic acid [5].


References
- AlamMS,ShriraoN.Giantmolluscumcontagiosumpresentingaslid neoplasm in an immunocompetent child. Dermatol Online J. 2016; 22.
- Pandhi D, Singhal A. Giant molluscum contagiosum. Indian Pediatr. 2005; 42(5): 488-9.
- Vozmediano JM, Manrique A, Petraglia S, Romero MA, Nieto I. Giant molluscum contagiosum in AIDS. Int J Dermatol. 1996; 35(1): 45-7.
- Alrajeh M, Alessa D, Maktabi AM, Al Alsheikh O. Eyelid molluscum contagiosum presenting as a giant solitary ulcerating mass. Saudi J Ophthalmol. 2018; 32: 338-40.
- Chen X, Anstey AV, Bugert JJ. Molluscum contagiosum virus infection. Lancet Infect Dis. 2013; 13(10): 877-88.