
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Delayed awakening due to extradural hematoma after intracranial cyst surgery: A case report
Gopinath Reddy1 ; Swati Vijapurkar2 *; Mayank Kumar3 ; G Sai Mahitha4 ; Sravani Jakkireddy4
1Junior Resident, All India Institute of Medical Sciences, Raipur, India.
2PDCC Neuroanesthesia, All India Institute of Medical Sciences, Raipur, India
3Additional Professor, Department of Anaesthesia, All India Institute of Medical Sciences, Raipur, India.
4Senior Resident, All India Institute of Medical Sciences, Raipur, India.
*Corresponding Author : Swati Vijapurkar
PDCC Neuroanesthesia, All India Institute of
Medical Sciences, Raipur, India.
Tel: 9901967469,
Email: swativijapurkar24@gmail.com
Received : Mar 03, 2025
Accepted : Mar 24, 2025
Published : Mar 31, 2025
Archived : www.jcimcr.org
Copyright : © Vijapurkar S (2025).
Abstract
Delayed awakening following neurosurgery is a multifactorial condition requiring a structured and timely evaluation. It poses diagnostic and management challenges, requiring prompt identification of reversible causes to optimize patient outcomes. It may result from various factors, including anesthetic effects, metabolic disturbances, structural brain injuries, or complications such as hydrocephalus and seizures. Surgical factors require quick evaluation via neuroimaging like computed tomography. An extradural hematoma may develop after decompression of a large intracranial cyst or tumor that may predispose to delayed awakening. Early identification and management of treatable causes are essential to improving patient outcomes.
Keywords: Hematoma; Decompression; Neuroimaging; Cyst.
Citation: Reddy G, Vijapurkar S, Kumar M, Mahitha SG, Jakkireddy S. Delayed awakening due to extradural hematoma after intracranial cyst surgery: A case report. J Clin Images Med Case Rep. 2025; 6(3): 3531.
Introduction
Early emergence after neurosurgery is desirable to facilitate neurological examination and early identification of complications [1]. Awakening is determined by many factors including preoperative status, type of surgery, respiratory failure, metabolic derangements, intraoperative events and neurological complications [2]. Extradural hematoma (EDH) is a rare complication after intracranial tumor resection or cyst decompression. Here we describe a case report of the development of an unanticipated EDH after the decompression of a large intracranial cyst which resulted in delayed awakening.
Case report
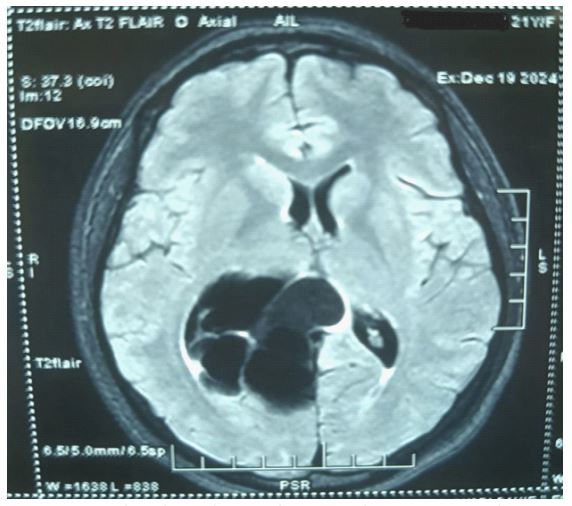
A 21-year-old female weighing 51 kilograms, with no significant past/medical history presented to the emergency department with chronic headache for 1 month, sudden onset 1 episode of general tonic clonic seizures, and 2 episodes of vomiting one day back. General examination was unremarkable with a glasgow coma score of 15 and stable vitals. The biochemical investigations were within normal limits. Magnetic resonance imaging (MRI) revealed a well-defined multiloculated arachnoid cyst with multiple thin septations measuring 6.2×4.5×5.5 cm located in the periatrial region of the right lateral ventricle (Figure 1).
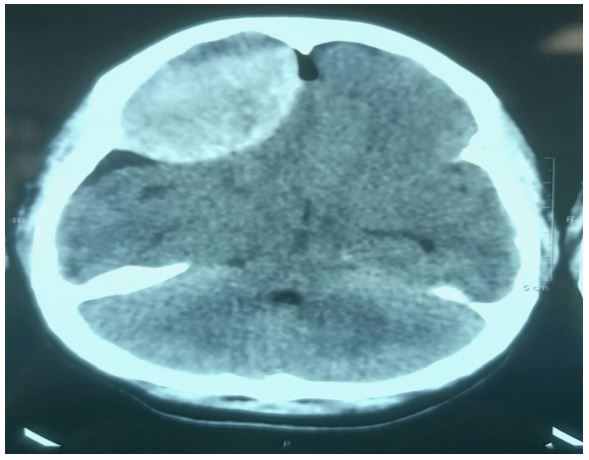
The patient was scheduled for parieto-occipital craniotomy and cyst decompression under general anesthesia. After confirming a fasting status of 6 hours the patient was taken into the operation room. Standard American Society of Anesthesiologists (ASA) monitors were attached, an arterial line secured in the right radial artery and a 16 gauge wide bore intravenous catheter was secured. The patient was positioned supine with the head secured in Mayfield head holder pins. Intraoperatively, the patient’s vital signs remained stable, parieto-occipital craniotomy was performed and cyst decompression was uneventful. In the immediate postoperative period, the patient exhibited poor GCS and no awakening despite complete wash out of the anaesthetic agents and complete reversal of neuromuscular blockade. The patient exhibited signs of raised intracranial pressure, elevated blood pressure, bradycardia and altered breathing pattern (Figure 2). A Computed Tomography (CT) scan identified a frontal extradural hematoma (EDH) (Figure 3), which was promptly evacuated via frontal craniotomy. The patient was intubated overnight for monitoring and successfully extubated the following morning.

Discussion
Extradural (epidural) hematoma is a collection of blood between the dura mater and the inner surface of the skull, usually caused by head trauma following road traffic accidents that results in arterial bleeding, often from the middle meningeal artery [3]. Skull fractures especially of the temporal bone often damages the middle meningeal artery leading to EDH. The expanding hematoma increases the intracranial pressure, which may lead to uncal herniation through the tentorial notch. The oculomotor nerve is compressed against the edge of the tentorium causing pupil dilation (blown pupil). This suggests impending brainstem compression and requires immediate surgical intervention to prevent death [4]. Delayed awakening in neurosurgical patients may result from primary neurological causes like intracranial hemorrhage, cerebral hematoma, hydrocephalus, convulsions/non-convulsive seizures or stroke. These conditions result in raised intracranial pressure and alter consciousness, which may predispose to delayed awakening. Metabolic and systemic causes like hypoxia, hypo/hypercarbia, electrolyte disturbances like hyper/hyponatremia, hypoglycemia, hypothermia and residual anesthetic/sedative effects are other causes of delayed awakening [5].
This case presented the difficulty in differential diagnosis of delayed awakening and the evaluation for the cause in a seemingly uncomplicated neurosurgical procedure. Management involves addressing the underlying cause, surgical evacuation of hematoma if present, correction of metabolic imbalances, reversal of residual anesthesia or neuromuscular blockade, antiepileptic treatment if seizures are detected, oxygenation and ventilation support if needed. Clinical examination involves analysing glasgow coma scale (GCS), pupillary response, brainstem reflexes and motor responses (spontaneous or to stimuli). Immediate investigations that can be done are CT brain to rule out hemorrhage, stroke, or hydrocephalus [6]. Arterial Blood Gas (ABG) to assess oxygenation, CO₂ retention, and acid-base status; serum electrolytes and glucose [7].
In our patient, delayed awakening was caused by surgical complications. Remote EDH is defined when an EDH occurs at a site away from the primary surgical site. The sudden and drastic fluctuations of intracranial pressure (ICP) results in the EDH [8]. This fluctuation may result from large tumor resection or rapid release of CSF and sac fluid. In our case, after evacuation of the large cyst following parieto-occipital craniotomy, there seemed to occur ‘brain-fall’ that may have led to the stripping of the dura from the skull at the frontal region. Patients of the younger age group have less tight adhesions between the dura and the skull which may be a contributing factor, since our patient was 21-years-old [9]. A case report of three remote epidural hematomas after craniotomy with similar mechanisms were reported [10]. In a retrospective analysis of 14 cases of remote epidural hematoma as a postoperative complication after intracranial tumor resection, the incidence of postoperative remote EDH after intracranial tumor resection was reported to about 0.15% [8]. Fracture of the skull at the site of the Mayfield head holder may also cause an EDH [11], but this was rules out in our case.
The EDH thus led to the raised ICP and delayed awakening of the patient. The confirmation of the EDH was done by CT scan. In the early postoperative period, every patient with neurological deterioration or not waking up from anesthesia should have a rapid cranial CT scan because early detection and removal of postoperative acute EDH can be life-saving.
Conclusion
This case emphasizes the importance of vigilant postoperative monitoring for complications such as EDH, even after seemingly routine neurosurgical procedures. It also highlights the need for tailored anesthesia management, early recognition of treatable causes and appropriate management in patients undergoing complex neurosurgical interventions to improve outcomes.
Author contributions:
Concept and design: Gopinath Reddy, Swati Vijapurkar, G Sai Mahitha
Acquisition, analysis, or interpretation of data: Gopinath Reddy, Swati Vijapurkar, Sravani Jakkireddy
Drafting of the manuscript: Gopinath Reddy, Swati Vijapurkar, Mayank Kumar
Critical review of the manuscript for important intellectual content: Mayank Kumar, G Sai Mahitha, Sravani Jakkireddy
Supervision: Swati Vijapurkar, Mayank Kumar, G Sai Mahitha
References
- Prabhakar H, Singh GP, Mahajan C, Kapoor I, Kalaivani M, Anand V. Intravenous versus inhalational techniques for rapid emergence from anaesthesia in patients undergoing brain tumour surgery. Cochrane Database Syst Rev. 2016; 9(9): CD010467. doi: 10.1002/14651858.CD010467.pub2. PMID: 27611234; PMCID: PMC6457852.
- Bhairwa, Devendra P, Kapil, Sonia; Mahajan, Shalvi, et al,. Factors Affecting Time to Emergence From General Anesthesia Following Clipping of Ruptured Aneurysms: A Prospective Observational Study. Neurology India. 2021; 69(5): 1302-1308. | DOI: 10.4103/0028-3886.329619
- Khairat A, Waseem M. Epidural Hematoma [Internet]. National Library of Medicine. StatPearls Publishing; 2023.
- Knight J, Rayi A. Transtentorial Herniation [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2021.
- Misal US, Joshi SA, Shaikh MM. Delayed recovery from anesthesia: A postgraduate educational review. Anesth Essays Res. 2016; 10(2): 164-72. doi: 10.4103/0259-1162.165506. PMID: 27212741; PMCID: PMC4864680.
- Unnithan AKA, Mehta P, Das JM. Hemorrhagic Stroke [Internet]. National Library of Medicine. Treasure Island (FL): StatPearls Publishing; 2023.
- Shao R, Liu L, Xu J, Lan P, Wu G, Shi H, Li R, Zhuang Y, Han S, Li Y, Zhao P, Xu M, Tang Z. Acidosis in arterial blood gas testing is associated with clinical outcomes after endovascular thrombectomy. Front Neurol. 2022; 13: 1077043. doi: 10.3389/ fneur.2022.1077043. PMID: 36619912; PMCID: PMC9811946.
- Yu J, Yang H, Cui D, Li Y. Retrospective analysis of 14 cases of remote epidural hematoma as a postoperative complication after intracranial tumor resection. World J Surg Oncol. 2016; 14: 1. doi: 10.1186/s12957-015-0754-8.
- Cui Z, Zhong C, Zhang M, Wu Z, Xu S, Zheng Y, Luo Q, Jiang J. Remote epidural haematoma and severe basal ganglia oedema complicating the removal of a central neurocytoma in the lateral ventricle: a case report and lessons learned. Clin Neurol Neurosurg. 2013; 115: 365–367. doi: 10.1016/j.clineuro.2012.05.043.
- Chung HJ, Park JS, Park JH, Jeun SS. Remote postoperative epidural hematoma after brain tumor surgery. Brain Tumor Res Treat. 2015; 3: 132–7. doi: 10.14791/btrt.2015.3.2.132.
- Naik V, Goyal N, Agrawal D. Pin site bilateral epidural hematoma - a rare complication of using Mayfield clamp in neurosurgery. Neurol India. 2011; 59: 649–651. doi: 10.4103/0028- 3886.84368.