
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 6
Massive skin and visceral involvement in diffuse large B cell lymphoma: Report of a rare illustrative case with a literature review
*Corresponding Author : Houda Benider
Faculty of Medicine and Pharmacy, University Hassan II, Casablanca, Morocco.
Email: beniderhouda@gmail.co
Received : Mar 05, 2025
Accepted : Mar 25, 2025
Published : Apr 01, 2025
Archived : www.jcimcr.org
Copyright : © Benider H (2025).
Abstract
A massive skin and multi visceral involvement of large B-cell lymphoma is a rare type of non-Hodgkin lymphomas. A 71-year-old man had multiple painless, reddish and firm cutaneous-subcutaneous nodules and masses on his chest and his back, gradually increasing in size. Skin biopsy result was consistent with diffuse large B-cell lymphoma. 18F-fluorodeoxyglycose (FDG). Positron Emission Tomography (PET) in combination with Computed Tomography (CT) (FDG PET/CT) was performed for staging and demonstrated an increased FDG uptake in a massive cutaneous masses and a hypermetabolic multi visceral involvement. FDG PET/CT is an essential tool for staging and mapping the disease, therefore an appropriate therapeutic strategy could be chosen, enabling patients to be treated appropriately and effectively.
Keywords: Case report; DLBCL; PET-CT FDG; Nuclear medicine.
Citation: Benider H. Massive skin and visceral involvement in diffuse large B cell lymphoma: Report of a rare illustrative case with a literature review. J Clin Images Med Case Rep. 2025; 6(4): 3533.
Introduction
Diffuse Large B-Cell Lymphoma (DLBCL) represents the most common subtype of non- Hodgkin lymphoma, accounting for 30% to 40% of all newly diagnosed cases [1]. Positron Emission Tomography (PET) is a nuclear imaging technique in which radiotracers suchas 11C and 18F are used. 18F-Fluoro-deoxyglycose (18F-FDG) - Positron Emission Tomography (PET) incombination with Computed Tomography (CT) (FDG PET/CT) has been proved over the years avaluable tool for the staging of aggressive lymphomas. Compared with conventional nuclear imaging, PET has a higher sensitivity and spatial resolution, mainly due to the concept of coincidence detection [2]. The consensus guidelines from the International Conference on Malignant Lymphoma in Lugano recommend staging with PET-CT for all the lymphomas avid to 18F-FDG [3,4]. In these guidelines, PET-CT was more accurate than CT for staging aggressive lymphomas, especially for the detection of the extra nodal disease. Due to its superior sensitivity in the detection of nodal and extra-nodal lymphoma manifestations, FDG PET/CT is strongly recommended for staging patients with DLBCL [5].
We report the clinical observation of a patient with a rare massive skin and multi- visceral involvement of DLBCL that illustrates the diagnostic role of FDG PET/CT in the initial staging.
Case presentation
A 71 years old man manifesting multiple painless, reddish and firm cutaneous- subcutaneous nodules and masses on his chest and his back, gradually increasing in size, combined with erythematous patches and collateral circulation (Figure 1).
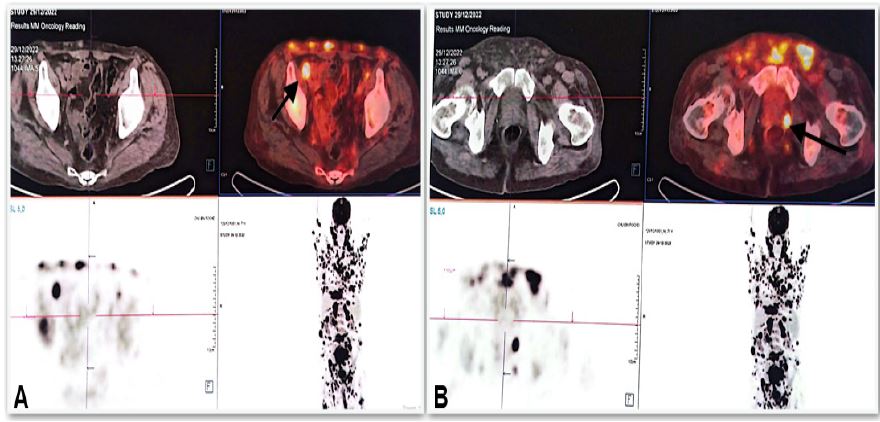
He also presented a bilateral axillary swelling. Skin biopsy result was consistent with a diffuse large B cell lymphoma. A F-18 Fluorodeoxyglucose Positron Emission Tomography and Computed Tomography (FDG PET/CT) was performed for initial staging and showed a massive supra- and sub- diaphragmatic lymph node involvement (cervical bilateral, axillary bilateral, mediastinal,peritoneal and pelvic) (Figure 2).
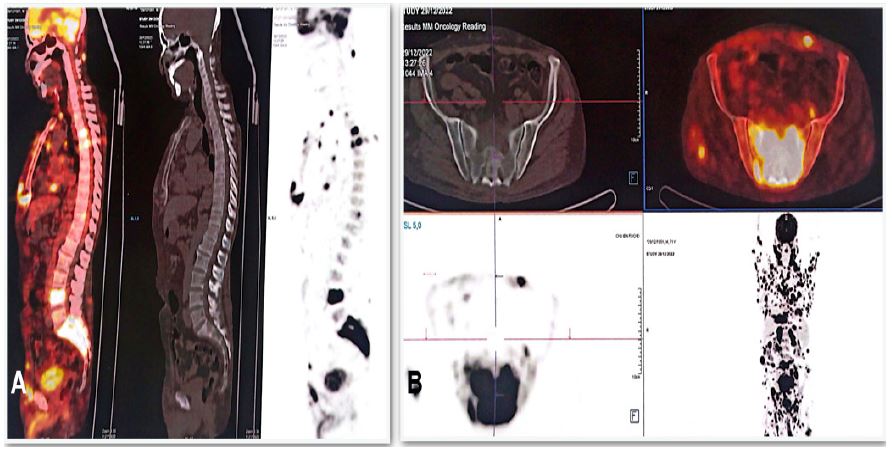
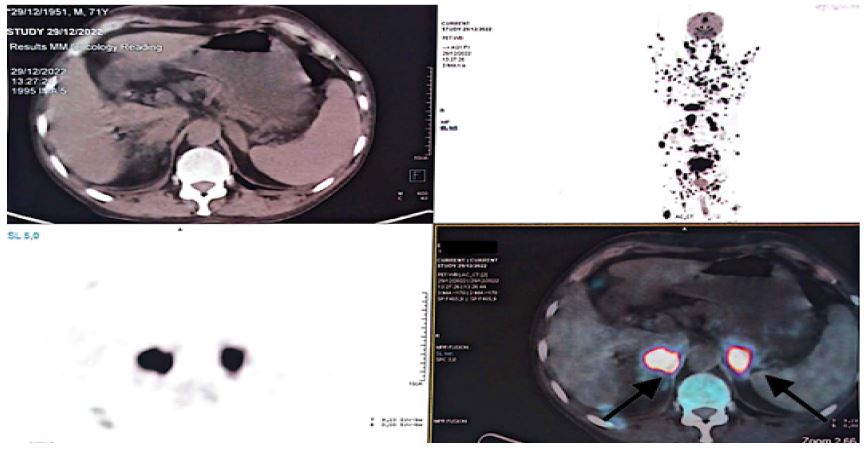
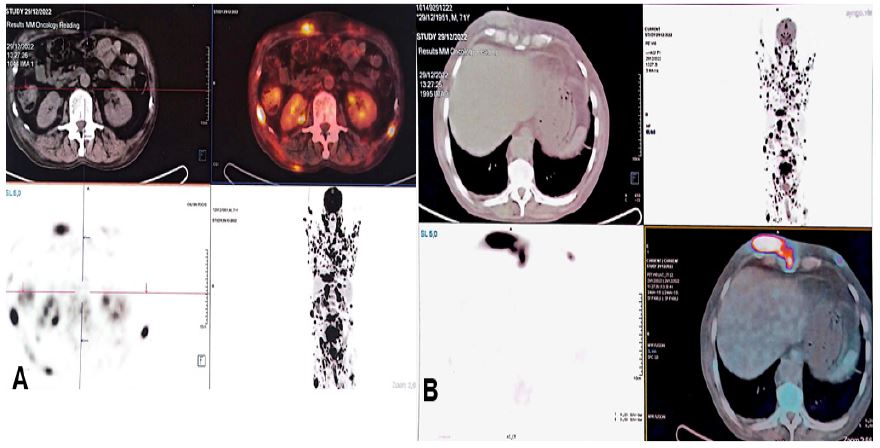
PET, CT, and fused PET/CT images showing a lymph node involvement in the left peri-prostatic area (arrow) and a multiple cutaneous and subcutaneous masses in the pelvic wall. It showed also a multi-visceral involvement in the brain, thyroid, heart, pleura, stomach,osseous (Figure 3), adrenal glands (Figure 4), kidney, muscles and cutaneous (Figure 5). Thus, the patient was diagnosed as stage IV of Ann Arbor because of the multi- visceral involvement, which is an advanced stage of the disease.

Discussion
FDG PET/CT has been demonstrated to be an irreplaceable tool for staging of a non- Hodgkin lymphoma, especially in DLCBL which is an aggressive lymphoma and very avidto FDG. The sensitivity of FDG PET/CT in the staging of DLBCL has been proven in a study tobe up to 97% [6]. A retrospective Chinese study of Shi and al [7], evaluating 1085 patients with DLBCL, showed in staging by FDG PET/CT an extra nodal involvement in 37,4% of cases andthe most common sites were stomach, intestine, nose, testis, skin, thyroid, central nervous system, breast and bone, which are sites that are almost similar to our case. Another retrospective study of Kaddu-Mulindwa and al [8] based on two multicentral studies OPTIMAL>60 and PETAL with a total number of patients of 903 with non-Hodgkin lymphoma (96% had DLBCL) that undergone a FDG PET/CT for staging that showed an advanced stage in 54% cases and an extra nodal involvement in 30% of all patients.
A recent prospective registry data support about FDG PET/CT staging strategy in aggressive non-Hodgkin lymphoma [9]. About 520 patients with early-stage aggressive non-Hodgkin lymphoma or with findings that were equivocal for advanced stage disease following clinical and CT assessment were restaged on the basis of FDG PET/CT. PET- CT upstaged 92 (28%) of 326 patients with apparent early-stage disease and reclassified108 (56%) of 194 patients with equivocal findings as advanced disease. Therefore, a significant change in the number of disease management strategies was statistically proven, 353 patients with planned treatment using CT were restaged by PET- CT. Around 40% (57 cases of 144 patients planned for combined modality treatment with CT were reassigned to receive chemotherapy alone, and 28% (44 of 156 patients) planned for chemotherapy were reassigned to receive combined modality treatment. The 1-year mortality rate for patients with early-stage disease defined by PET-CT was 6% comparedwith 14.2% for their counterparts assessed with CT. This result suggests that PET- directed management improved overall survival in patients and that was not only because of stage migration [10].
Conclusion
FDG PET/CT is an essential tool in staging of DLBCL, and several studies have demonstrated its superiority over CT, enabling the upstaging or reclassification of severalpatients. This has an impact on therapeutic strategy, enabling patients to be treated appropriately and effectively, and furthermore improving overall survival. The role of FDGPET/CT has not yet been precisely demonstrated and codified in therapeutic evaluation as in Hodgkin lymphoma, but several promising studies are underway.
Consent statement and declaration of interest: The authors have no conflicts of interest to declare. All co-authors have seen and agree with the contents of the manuscript and there is no financial interest to report. We certify that the submission is original work and is not under review at any other publication.
References
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, et al. WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues, Review 4th ed.; International Agency for Research on Cancer: Lyon, France. 2017.
- Shukla AK, Kumar U. Positron emission tomography: An overview. J Med PhysicsAssociation Med Phys India. 2006; 31(1): 13.
- Chesson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lu- gano classification. J Clin Oncol. 2014; 32(27): 3059-3068.
- Barrington SF, Mikhaeel NG, Kostakoglu L, et al. Role of imaging in the staging and response assessment of lymphoma: consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J Clin Oncol. 2014; 32(27): 3048-3058.
- Gómez León N, Delgado-Bolton RC, Del Campo Del Val L, Cabezas B, Arranz R, et al. Multicenter comparison of contrast- enhanced FDG PET/CT and 64-slice multi-detector-row CT for initial staging and response evaluation at the end of treatment in patients with lymphoma. Clin. Nucl. Med. 2017; 42: 595-602.
- Barrington SF, Mikhaeel NG, Kostakoglu L, Meignan M, Hutchings M, et al. Role of imaging in the staging and response assessment of lymphoma: consensus of the International Conference on Malignant Lymphomas Imaging Working Group. Journal of clinical oncology. 2014; 32(27): 3048.
- Shi Y, Han Y, Yang J, Liu P, He X, et al. Clinical features and outcomes of diffuse large B-cell lymphoma based on nodal or extranodal primary sites of origin: Analysis of 1,085 WHO classified cases in a single institution in China. Chinese journal of cancer research. 2019; 31(1): 152.
- Kaddu-Mulindwa D, Altmann B, Held G, Angel S, Stilgenbauer S, Thurner L, et al. FDG PET/CT to detect bone marrow involvement in the initial staging of patients with aggressive non-Hodgkin lymphoma: Results from the prospective, multicenter PETAL and OPTIMAL> 60 trials. European journal of nuclear medicine and molecular imaging. 2021; 48(11): 3550-3559.
- Metser U, Prica A, Hodgson DC, et al. Effect of PET/CT on the management and outcomes of participants with Hodgkin and aggressive non-Hodgkin lymphoma: a multicenter registry. Radiology 2019; 290: 488-95.
- Barrington SF, & Trotman J. The role of PET in the first-line treatment of the most common subtypes of non-Hodgkin lymphoma. The Lancet Haematology. 2021; 8(1): 80-93.